

Evaluation of the Pharmacokinetics and Exposure-Response Relationship of Dapagliflozin in Patients without Diabetes and with Chronic Kidney Disease
- PMID: 33587286
- PMCID: PMC8016788
- DOI: 10.1007/s40262-020-00956-1
Evaluation of the Pharmacokinetics and Exposure-Response Relationship of Dapagliflozin in Patients without Diabetes and with Chronic Kidney Disease
Abstract
Background and objective: Dapagliflozin, a sodium-glucose co-transporter inhibitor, was originally developed as an oral glucose-lowering drug for the treatment of type 2 diabetes mellitus. Emerging data suggest that cardiovascular and kidney benefits extend to patients without diabetes. Limited pharmacological data are, however, available in patients without diabetes. We aimed to characterise the pharmacokinetic profile of dapagliflozin in patients with chronic kidney disease without type 2 diabetes.
Methods: Plasma samples were collected in a randomised, placebo-controlled, double-blind, cross-over trial (DIAMOND, NCT03190694, n = 53) that assessed the effects of 10 mg of dapagliflozin in patients with a glomerular filtration rate ≥ 25 mL/min/1.73 m2 and proteinuria > 500 mg/day. Mixed-effects models were used to develop a pharmacokinetic model and to evaluate the association between plasma exposure and response.
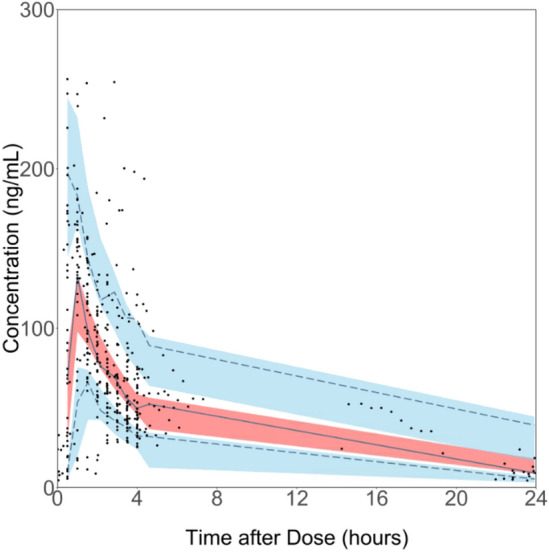
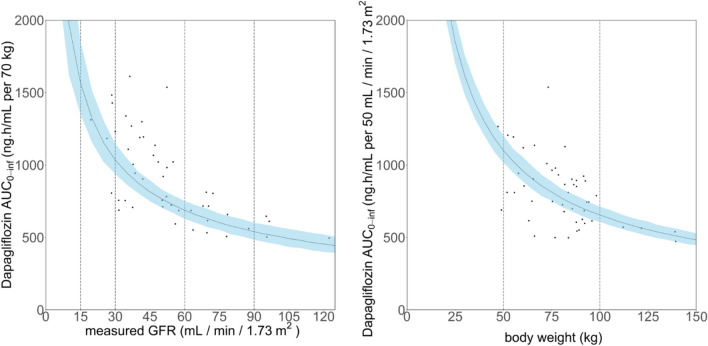
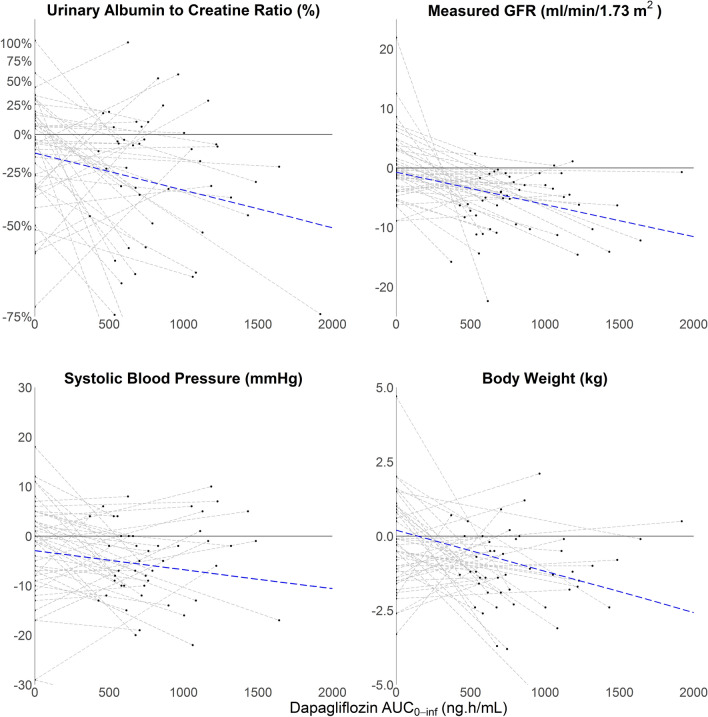
Results: Plasma concentrations (n = 430 observations) from 48 patients (mean age 50.8 years, mean glomerular filtration rate 57.9 mL/min/1.73 m2, median proteinuria 1115 mg/24 h) were best described using a two-compartment model with first-order elimination. Apparent clearance and volume of distribution were 11.7 (95% confidence interval 10.7-12.7) L/h and 44.9 (95% confidence interval 39.0-50.9) L, respectively. Median dapagliflozin plasma exposure was 740.9 ng h/mL (2.5th-97.5th percentiles: 434.0-1615.3). Plasma exposure increased with decreasing kidney function. Every 100-ng h/mL increment in dapagliflozin plasma exposure was associated with a decrease in the urinary albumin:creatinine ratio (β = - 2.8%, p = 0.01), glomerular filtration rate (β = - 0.5 mL/min/1.73 m2, p < 0.01) and systolic blood pressure (β = - 0.4 mmHg, p = 0.03).
Conclusions: The dapagliflozin plasma concentration-time profile in patients with non-diabetic kidney disease appears similar to the profile of patients with diabetic kidney disease described in the literature. Furthermore, the plasma exposure was associated with changes in risk markers for kidney disease.
Conflict of interest statement
Annemarie B. van der Aart-van der Beek, Abdul Halim Abdul Gafor, Claire C.J. Dekkers, Daniel C. Cattran, Jasper Stevens, Jeroen V. Koomen, Qiang Li, Sean J. Barbour and Sunita Singh have no conflicts of interest that are directly relevant to the content of this article. Hiddo J.L. Heerspink is a consultant to Abbvie, AstraZeneca, Boehringer Ingelheim, Bayer, Chinook, CSL Behring, Gilead, Janssen, Merck, Mundipharma, Mitsubishi Tanabe, Novo Nordisk and Retrophin. He received research support from AstraZeneca, Abbvie, Boehringer Ingelheim and Janssen. David W. Boulton is an employee and shareholder of AstraZeneca. David Z.I. Cherney has received honoraria from Boehringer Ingelheim-Lilly, Merck, AstraZeneca, Sanofi, Mitsubishi-Tanabe, Abbvie, Janssen, Bayer, Prometic, BMS and Novo-Nordisk and has received operational funding for clinical trials from Boehringer Ingelheim-Lilly, Merck, Janssen, Sanofi, AstraZeneca and Novo-Nordisk. Ron T. Gansevoort has consulting agreements with AstraZeneca, Bayer, Sanofi-Genzyme and Mundi Pharma; all fees are paid to his institution. Peter J. Greasley is employed by and owns shares in AstraZeneca. Gozewijn D. Laverman has received research grants and consulting fees from Sanofi and AstraZeneca, and research grants from Novo Nordisk. Marc G. Vervloet has received consulting fees from Amgen, Vifor, Fresenius Medical Care Renal Pharma, Medice, Kyowa Kirin and Astra Zeneca. Heather N. Reich has received consulting fees from Omeros and was involved in clinical trials supported by Omeros and Calliditas. Soo Kun Lim has received consulting fees or speaking honoraria from AstraZeneca, Boehringer Ingelheim, Novo Nordisk, Fresenius Kabi, Baxter and Sanofi.
Figures
References
-
- Heerspink HJ, Perkins BA, Fitchett DH, Husain M, Cherney DZ. Sodium glucose cotransporter 2 inhibitors in the treatment of diabetes mellitus: cardiovascular and kidney effects, potential mechanisms, and clinical applications. Circulation. 2016;134:752–772. doi: 10.1161/CIRCULATIONAHA.116.021887. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
