

Human Herpesvirus 6 Encephalitis in Immunocompetent and Immunocompromised Hosts
- PMID: 33587722
- PMCID: PMC7963435
- DOI: 10.1212/NXI.0000000000000942
Human Herpesvirus 6 Encephalitis in Immunocompetent and Immunocompromised Hosts
Abstract
Objective: The aim of this study was to analyze the clinical, radiologic, and biological features associated with human herpesvirus 6 (HHV-6) encephalitis in immunocompetent and immunocompromised hosts to establish which clinical settings should prompt HHV-6 testing.
Methods: We performed a retrospective research in the virology database of Fondazione IRCCS Policlinico San Matteo (Pavia, Italy) for all patients who tested positive for HHV-6 DNA in the CSF and/or in blood from January 2008 to September 2018 and separately assessed the number of patients meeting the criteria for HHV-6 encephalitis in the group of immunocompetent and immunocompromised hosts.
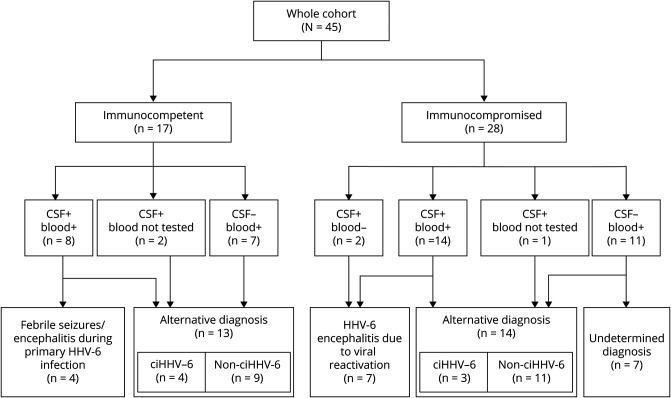
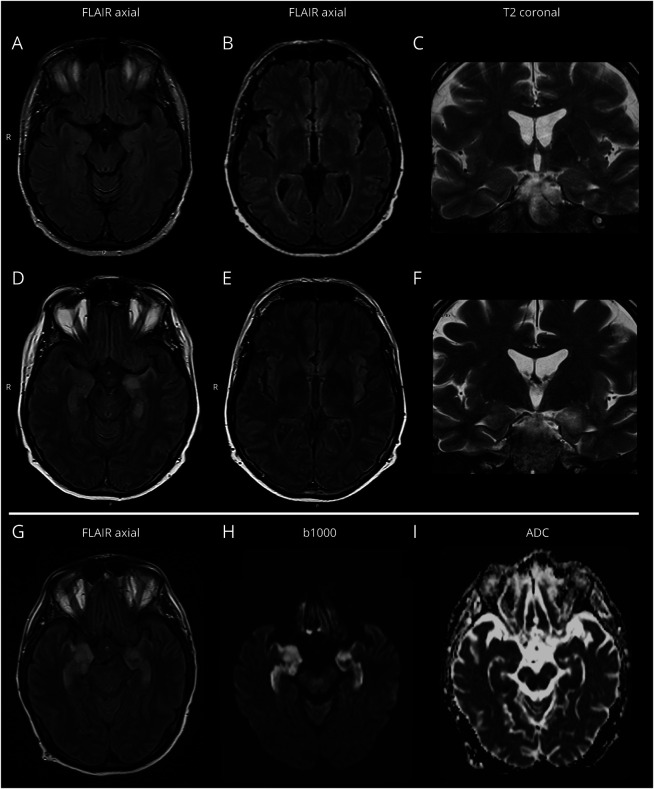
Results: Of the 926 patients tested for HHV-6 during the period of interest, 45 met the study criteria. Among immunocompetent hosts (n = 17), HHV-6 encephalitis was diagnosed to 4 infants or children presenting with seizures or mild encephalopathy during primary HHV-6 infection (CSF/blood replication ratio <<1 in all cases). Among immunocompromised hosts (n = 28), HHV-6 encephalitis was diagnosed to 7 adolescents/adults with hematologic conditions presenting with altered mental status (7/7), seizures (3/7), vigilance impairment (3/7), behavioral changes (2/7), hyponatremia (2/7), and anterograde amnesia (1/7). Initial brain MRI was altered only in 2 patients, but 6 of the 7 had a CSF/blood replication ratio >1.
Conclusions: The detection of a CSF/blood replication ratio >1 represented a specific feature of immunocompromised patients with HHV-6 encephalitis and could be of special help to establish a diagnosis of HHV-6 encephalitis in hematopoietic stem cell transplant recipients lacking radiologic evidence of limbic involvement.
Copyright © 2021 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Academy of Neurology.
Figures
Comment in
- Neurol Neuroimmunol Neuroinflamm. 96:e948.
References
-
- Agut H, Bonnafous P, Gautheret-Dejean A. Update on infections with human herpesviruses 6A, 6B, and 7. Med Mal Infect 2017;47:83–91. - PubMed
-
- Ward KN, Bryant NJ, Andrews NJ, et al. . Risk of serious neurologic disease after immunization of young children in Britain and Ireland. Pediatrics 2007;120:314–321. - PubMed
-
- Yoshikawa T, Ohashi M, Miyake F, et al. . Exanthem subitum-associated encephalitis: nationwide survey in Japan. Pediatr Neurol 2009;41:353–358. - PubMed
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous