

Increased Intracranial Hemorrhage Amid Elevated Inflammatory Markers in Those With COVID-19 Supported With Extracorporeal Membrane Oxygenation
- PMID: 33587724
- PMCID: PMC10763976
- DOI: 10.1097/SHK.0000000000001730
Increased Intracranial Hemorrhage Amid Elevated Inflammatory Markers in Those With COVID-19 Supported With Extracorporeal Membrane Oxygenation
Abstract
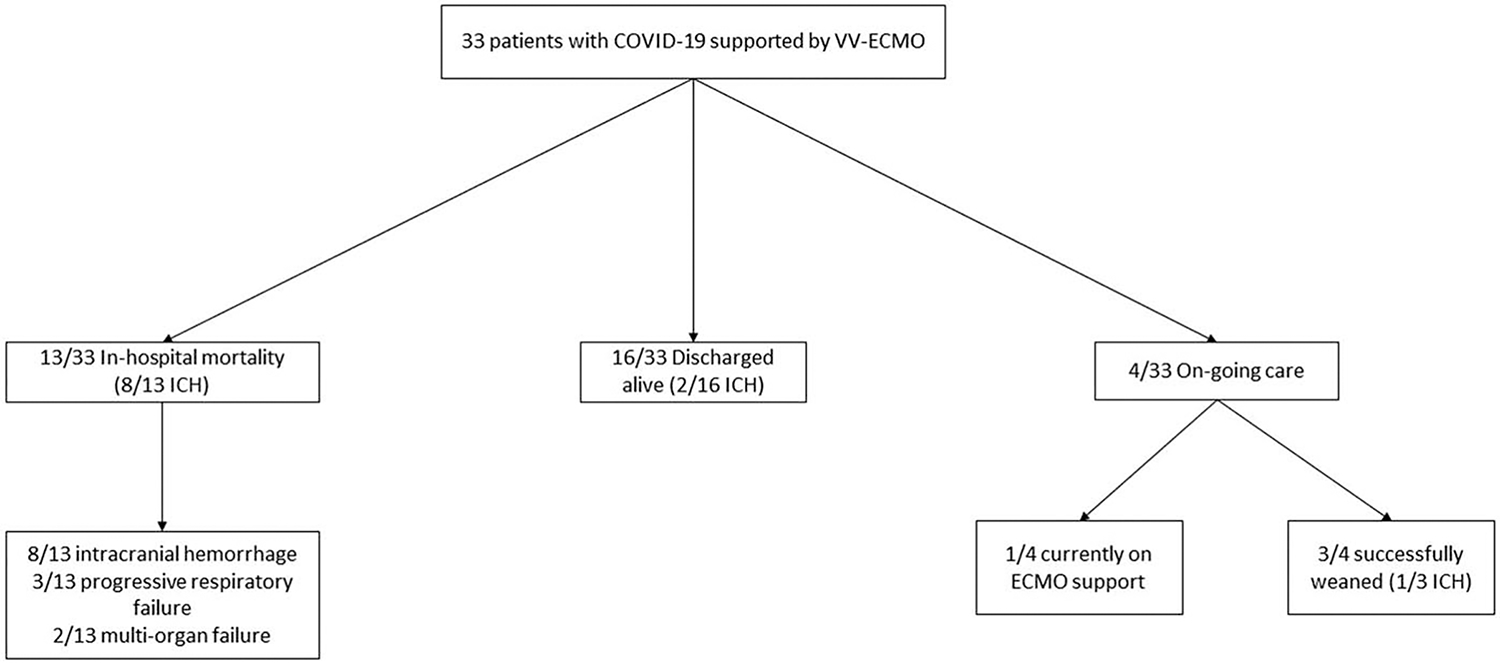
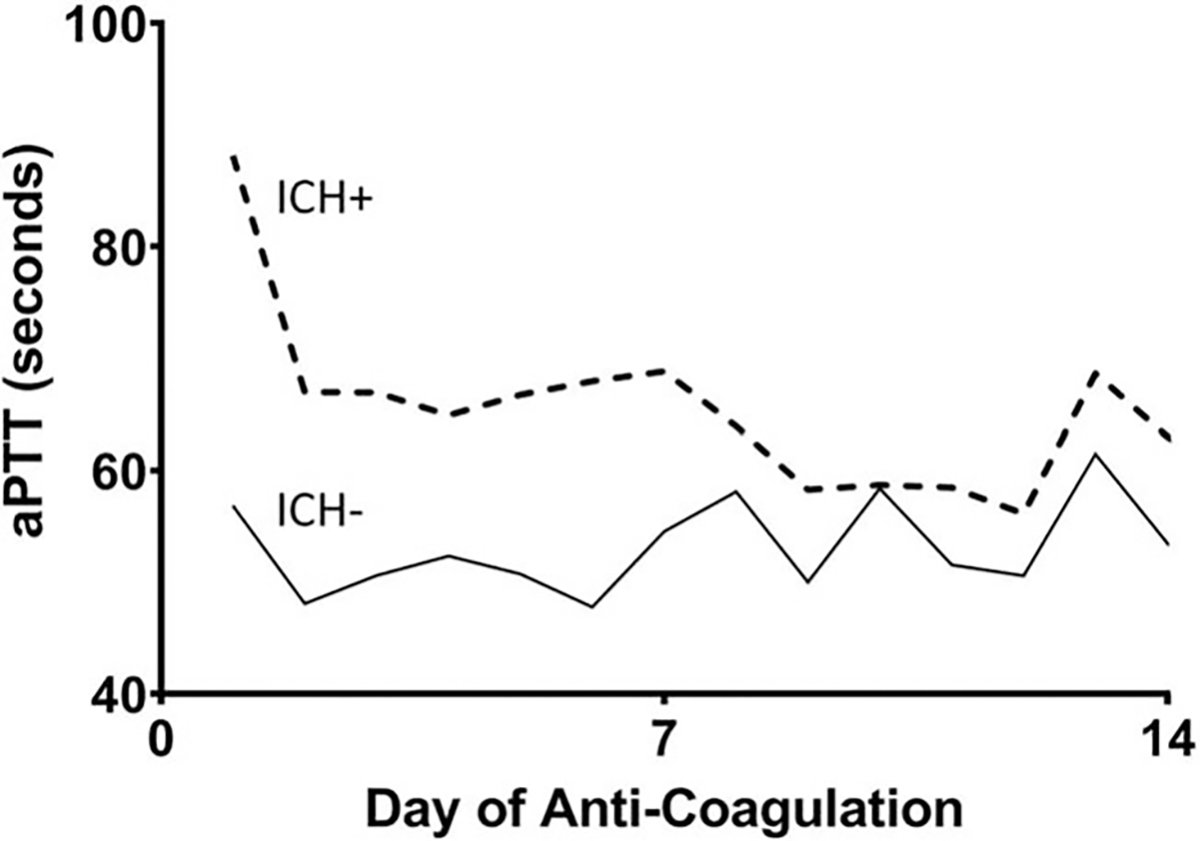
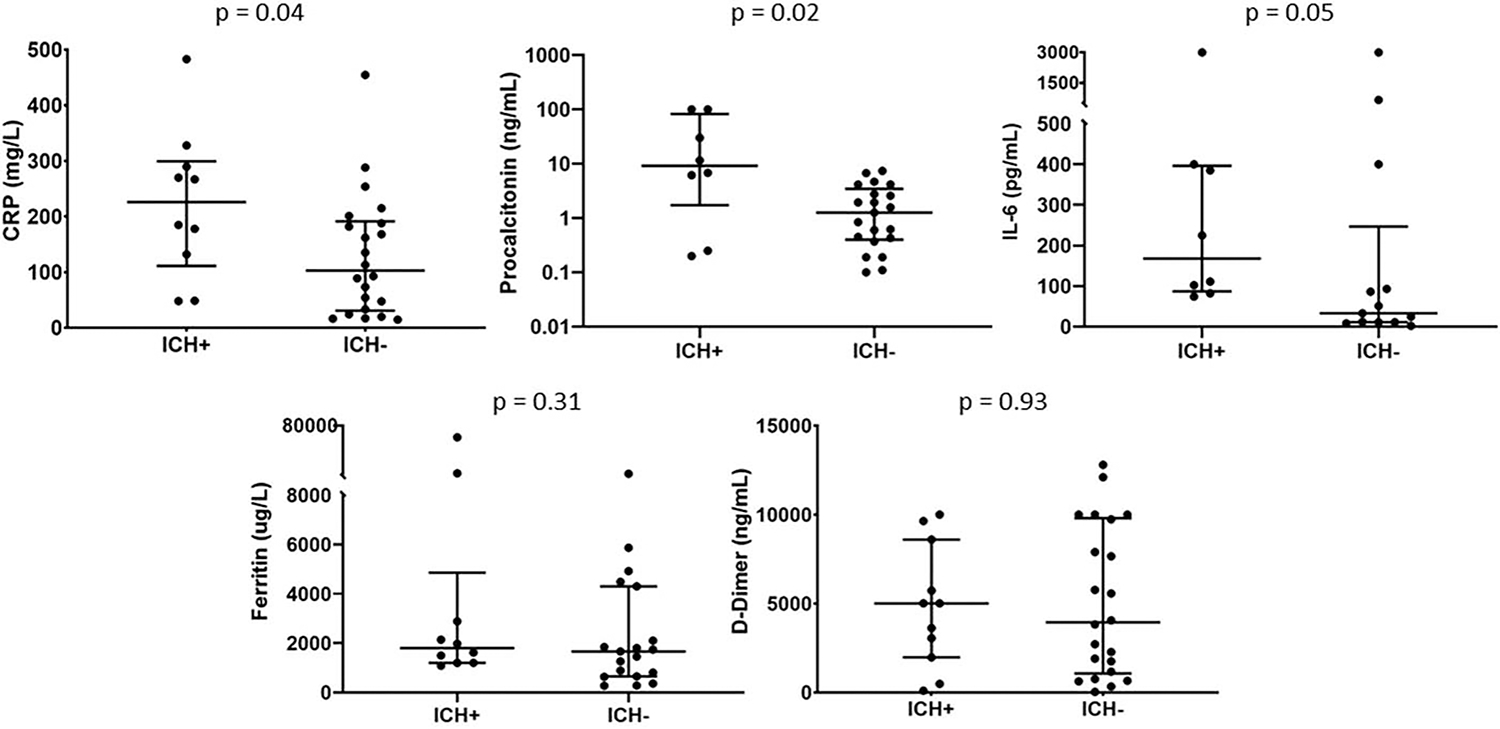
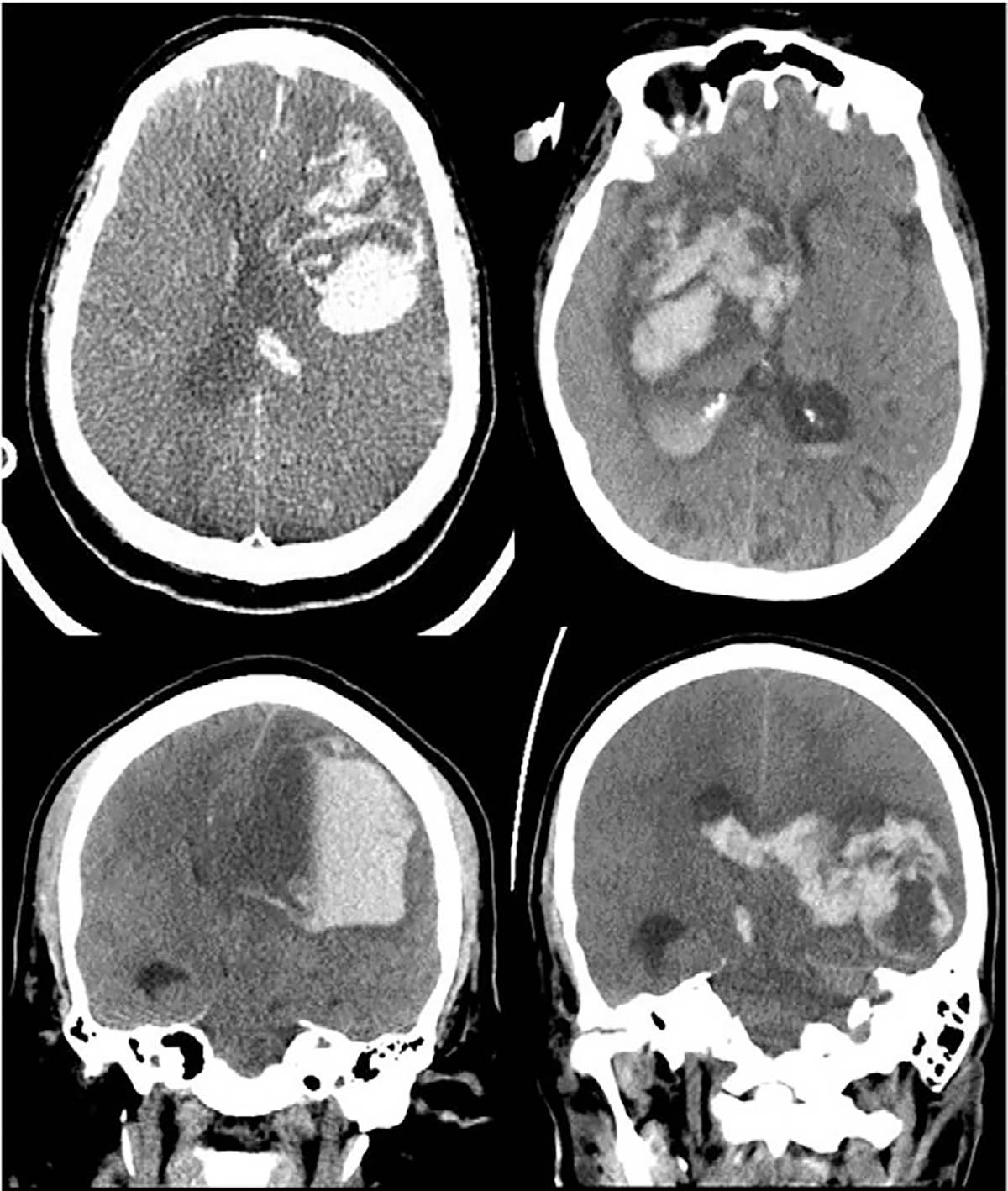
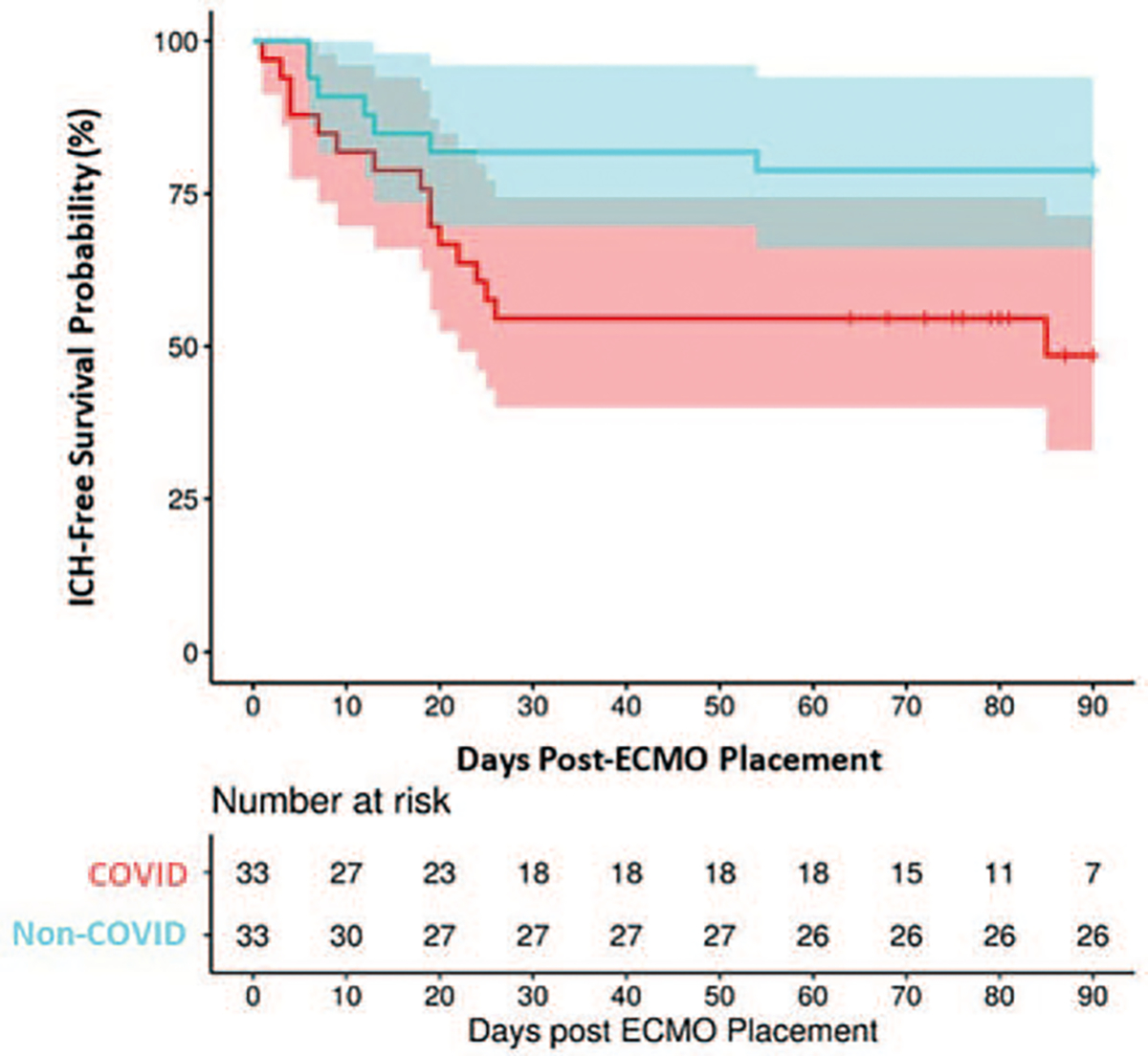
COVID-19-related coagulopathy is a known complication of SARS-CoV-2 infection and can lead to intracranial hemorrhage (ICH), one of the most feared complications of extracorporeal membrane oxygenation (ECMO). We sought to evaluate the incidence and etiology of ICH in patients with COVID-19 requiring ECMO. Patients at two academic medical centers with COVID-19 who required venovenous-ECMO support for acute respiratory distress syndrome (ARDS) were evaluated retrospectively. During the study period, 33 patients required ECMO support; 16 (48.5%) were discharged alive, 13 died (39.4%), and 4 (12.1%) had ongoing care. Eleven patients had ICH (33.3%). All ICH events occurred in patients who received intravenous anticoagulation. The ICH group had higher C-reactive protein (P = 0.04), procalcitonin levels (P = 0.02), and IL-6 levels (P = 0.05), lower blood pH before and after ECMO (P < 0.01), and higher activated partial thromboplastin times throughout the hospital stay (P < 0.0001). ICH-free survival was lower in COVID-19 patients than in patients on ECMO for ARDS caused by other viruses (49% vs. 79%, P = 0.02). In conclusion, patients with COVID-19 can be successfully bridged to recovery using ECMO but may suffer higher rates of ICH compared to those with other viral respiratory infections.
Copyright © 2021 by the Shock Society.
Conflict of interest statement
The authors report no conflicts of interest.
Figures
References
-
- Richardson S, Hirsch JS, Narasimhan M, Crawford JM, McGinn T, Davidson KW, Barnaby DP, Becker LB, Chelico JD, Cohen SL, et al.: Presenting characteristics, comorbidities, and outcomes among 5700 patients hospitalized with COVID-19 in the New York City Area. JAMA 323(20):2052–2059, 2020. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
