

Consensus on molecular imaging and theranostics in neuroendocrine neoplasms
- PMID: 33588146
- PMCID: PMC8903070
- DOI: 10.1016/j.ejca.2021.01.008
Consensus on molecular imaging and theranostics in neuroendocrine neoplasms
Abstract
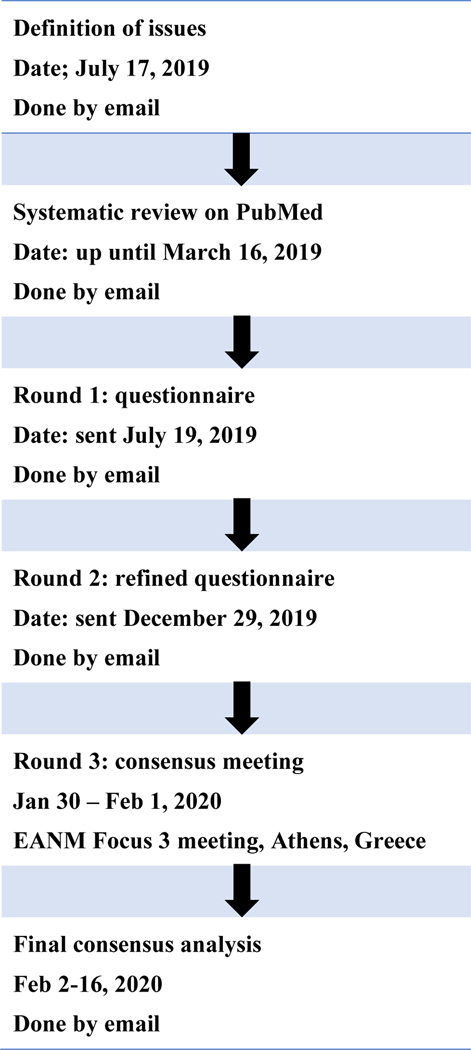
Nuclear medicine plays an increasingly important role in the management neuroendocrine neoplasms (NEN). Somatostatin analogue (SSA)-based positron emission tomography/computed tomography (PET/CT) and peptide receptor radionuclide therapy (PRRT) have been used in clinical trials and approved by the European Medicines Agency (EMA) and the US Food and Drug Administration (FDA). European Association of Nuclear Medicine (EANM) Focus 3 performed a multidisciplinary Delphi process to deliver a balanced perspective on molecular imaging and radionuclide therapy in well-differentiated neuroendocrine tumours (NETs). NETs form in cells that interact with the nervous system or in glands that produce hormones. These cells, called neuroendocrine cells, can be found throughout the body, but NETs are most often found in the abdomen, especially in the gastrointestinal tract. These tumours may also be found in the lungs, pancreas and adrenal glands. In addition to being rare, NETs are also complex and may be difficult to diagnose. Most NETs are non-functioning; however, a minority present with symptoms related to hypersecretion of bioactive compounds. NETs often do not cause symptoms early in the disease process. When diagnosed, substantial number of patients are already found to have metastatic disease. Several societies' guidelines address Neuroendocrine neoplasms (NENs) management; however, many issues are still debated, due to both the difficulty in acquiring strong clinical evidence in a rare and heterogeneous disease and the different availability of diagnostic and therapeutic options across countries. EANM Focus 3 reached consensus on employing 68gallium-labelled somatostatin analogue ([68Ga]Ga-DOTA-SSA)-based PET/CT with diagnostic CT or magnetic resonance imaging (MRI) for unknown primary NET detection, metastatic NET, NET staging/restaging, suspected extra-adrenal pheochromocytoma/paraganglioma and suspected paraganglioma. Consensus was reached on employing 18fluorine-fluoro-2-deoxyglucose ([18F]FDG) PET/CT in neuroendocrine carcinoma, G3 NET and in G1-2 NET with mismatched lesions (CT-positive/[68Ga]Ga-DOTA-SSA-negative). Peptide receptor radionuclide therapy (PRRT) was recommended for second line treatment for gastrointestinal NET with [68Ga]Ga-DOTA-SSA uptake in all lesions, in G1/G2 NET at disease progression, and in a subset of G3 NET provided all lesions are positive at [18F]FDG and [68Ga]Ga-DOTA-SSA. PRRT rechallenge may be used for in patients with stable disease for at least 1 year after therapy completion. An international consensus is not only a prelude to a more standardised management across countries but also serves as a guide for the direction to follow when designing new research studies.
Keywords: Consensus; Molecular imaging; Neuroendocrine neoplasms; PRRT.
Copyright © 2021 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Conflict of interest statement VA reports personal fees from ESMIT and AAA outside the submitted work and is a member of ENETS advisory board, ESMO faculty staff for NET and the scientific board of ITANET; JK reports personal fees from Bayer, outside the submitted work; LB reports non-paid consultant for AAA-Novartis, Ipson, Clovis Oncology, and Curium, and a research grant from AAA-Novaris; JC reports grants and personal fees from Bayer, Eisai, Advanced Accelerator Applications, and Ipsen, and grants from Astrazeneca, Novartis, Pfizer, Merck, Sanofi, Amgen, and Exelixis outside the submitted work; WDH reports personal fees and grants from Ipsen, personal fees from Novartis, and personal fees and grants, from AAA; CD reports consultancy/advisor for Ipsen; MaF reports personal fees from AAA, Novartis, Ipsen, and Celgene outside the submitted work; MeF reports personal fees and research funding from Ipsen; SF reports personal fees from ANMI, Astellas, Bayer, BlueEarth Diagnostics, GE Healthcare, Jenssen, Novartis, Sofie Biosciences, non-financial support from AAA, Bayer, GE Healthcare, Curium, Tema Sinergie, Sanofi, Telix, outside the submitted work; RJH reports holding shares in Telix Pharmaceuticals on behalf of his institution and receiving research funding from Ispen and ITM; VL reports advisory board member of AAA and Ipsen; DOT reports personal fees from Novartis, IPSEN, AstraZeneca and grants from Wyeth Lederle and Ipsen outside the submitted work; MP reports personal fees from AAA, Pfizer, and Riemser and grants and personal fees from Novartis and IPSEN outside the submitted work; RS reports consultancy for AAA, Ipsen, Novartis, ITM and Keocyt and participation in the NETTER 1 and COMPETE Trials; JS reports consultant for Novartis and speaker's bureau for Ipsen and Lexicon outside the submitted work; DT reports personal fees from AAA/Novartis, IPSEN and Sanofi-Genzyme, outside the submitted work; DW reports personal fees from Ipsen and grants form Siemens Healthineers and Debiopharm International S.A; KH reports personal fees from Bayer, other from Sofie Biosciences, personal fees from SIRTEX, non-financial support from ABX, personal fees from Adacap, personal fees from Curium, personal fees from Endocyte, grants and personal fees from BTG, personal fees from IPSEN, personal fees from Siemens Healthineers, personal fees from GE Healthcare, personal fees from Amgen, personal fees from Novartis, personal fees from ymabs, outside the submitted work; JY reports financial activities with Advanced Accelerated Applications (AAA), Chiasma, Crinetics, Hutchison MediPharma, Ipsen, Merck, Novartis, and Tarvedin. EB, CB, SM, MiC, MC, LK, GK, KO, WO, ASc, ASu, and IV declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
