

Electric field strength induced by electroconvulsive therapy is associated with clinical outcome
- PMID: 33588322
- PMCID: PMC7895836
- DOI: 10.1016/j.nicl.2021.102581
Electric field strength induced by electroconvulsive therapy is associated with clinical outcome
Abstract
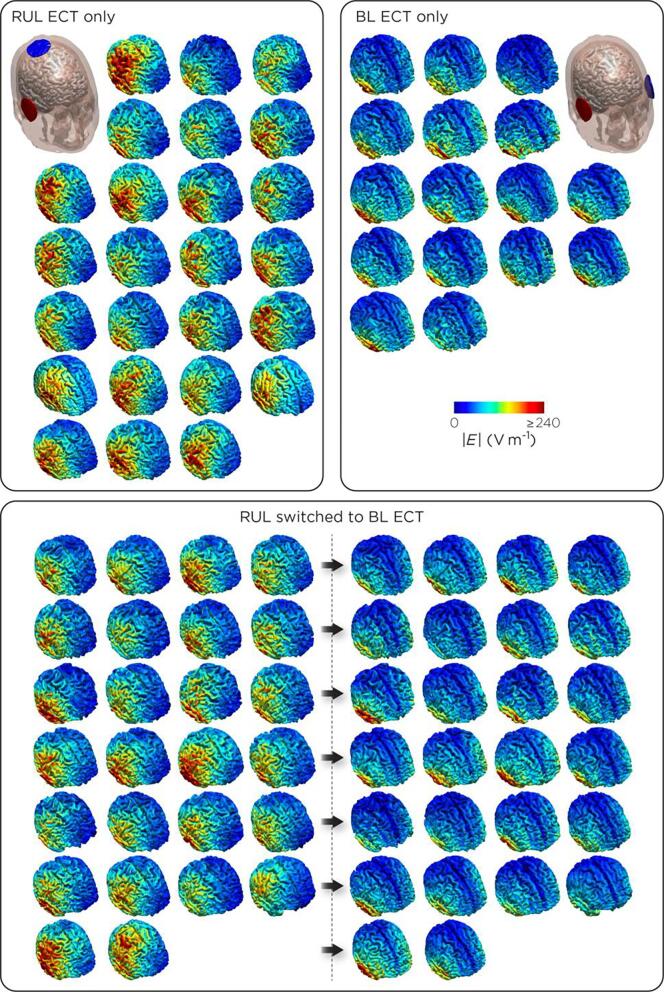
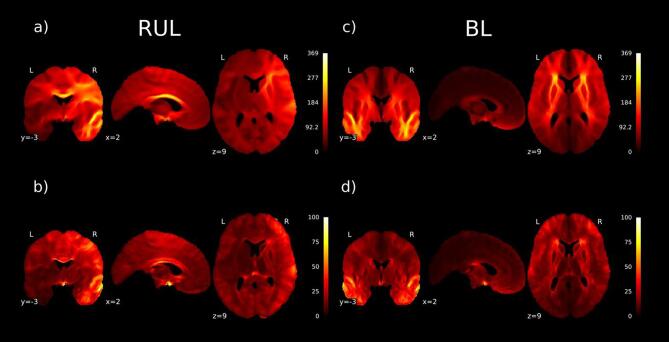
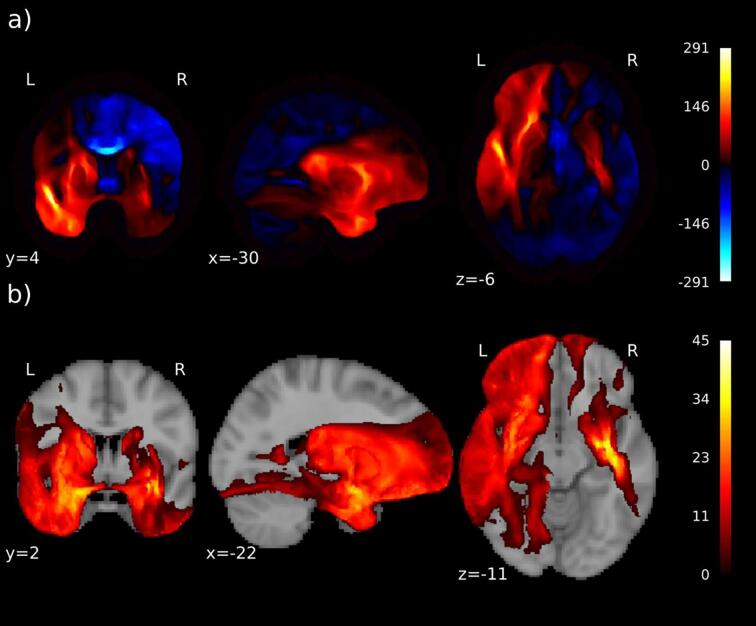
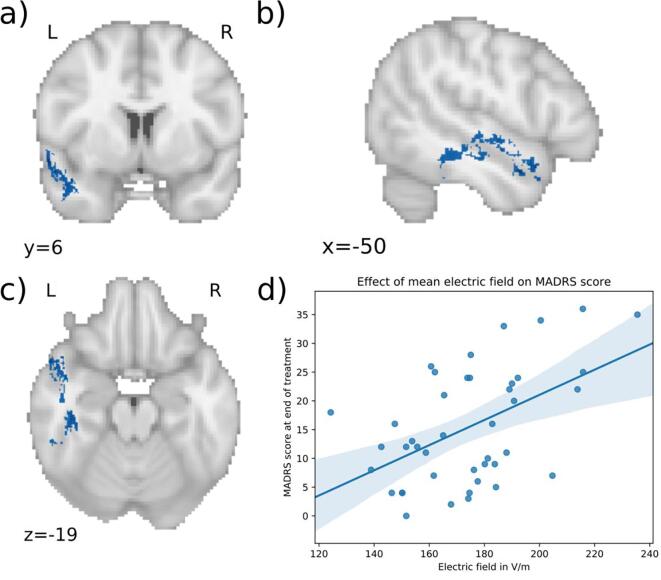
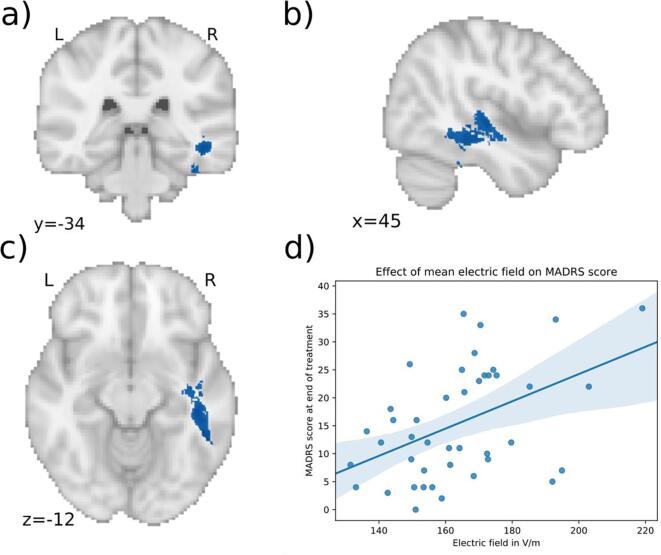
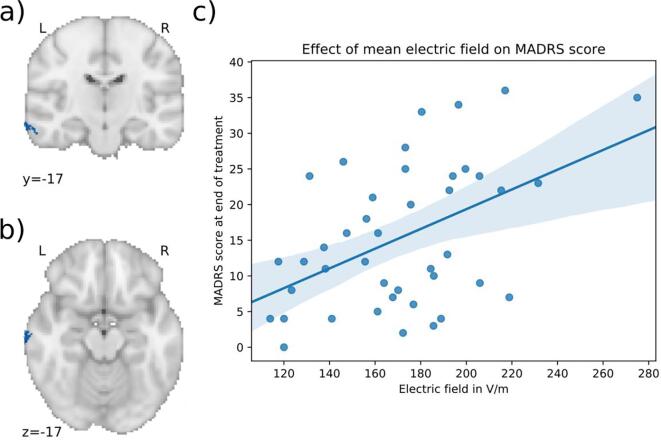
The clinical effect of electroconvulsive therapy (ECT) is mediated by eliciting a generalized seizure, which is achieved by applying electrical current to the head via scalp electrodes. The anatomy of the head influences the distribution of current flow in each brain region. Here, we investigated whether individual differences in simulated local electrical field strength are associated with ECT efficacy. We modeled the electric field of 67 depressed patients receiving ECT. Patient's T1 magnetic resonance images were segmented, conductivities were assigned to each tissue and the finite element method was used to solve for the electric field induced by the electrodes. We investigated the correlation between modelled electric field and ECT outcome using voxel-wise general linear models. The difference between bilateral (BL) and right unilateral (RUL) electrode placement was striking. Even within electrode configuration, there was substantial variability between patients. For the modeled BL placement, stronger electric field strengths appeared in the left hemisphere and part of the right temporal lobe. Importantly, a stronger electric field in the temporal lobes was associated with less optimal ECT response in patients treated with BL-ECT. No significant differences in electric field distributions were found between responders and non-responders to RUL-ECT. These results suggest that overstimulation of the temporal lobes during BL stimulation has negative consequences on treatment outcome. If replicated, individualized pre-ECT computer-modelled electric field distributions may inform the development of patient-specific ECT protocols.
Keywords: Electroconvulsive therapy; Finite element modelling; Major depressive disorder.
Copyright © 2021 The Author(s). Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
-
- Ustün T.B., Ayuso-Mateos J.L., Chatterji S., Mathers C., Murray C.J.L. Global burden of depressive disorders in the year 2000. Br. J. Psychiatry. 2004;184:386–392. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
