

Midterm outcome after posterior stabilization of unstable Midthoracic spine fractures in the elderly
- PMID: 33588814
- PMCID: PMC7885444
- DOI: 10.1186/s12891-021-04049-3
Midterm outcome after posterior stabilization of unstable Midthoracic spine fractures in the elderly
Abstract
Background: The evidence for the treatment of midthoracic fractures in elderly patients is weak. The aim of this study was to evaluate midterm results after posterior stabilization of unstable midthoracic fractures in the elderly.
Methods: Retrospectively, all patients aged ≥65 suffering from an acute unstable midthoracic fracture treated with posterior stabilization were included. Trauma mechanism, ASA score, concomitant injuries, ODI score and radiographic loss of reduction were evaluated. Posterior stabilization strategy was divided into short-segmental stabilization and long-segmental stabilization.
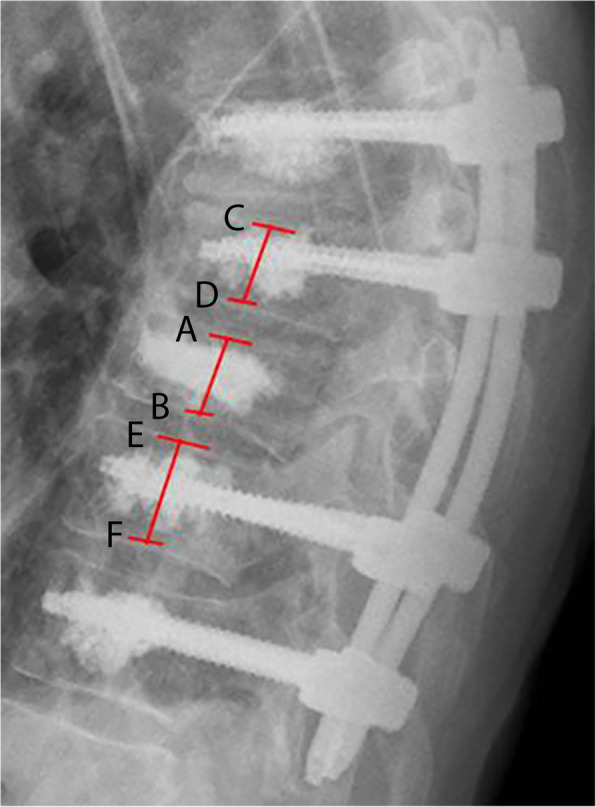
Results: Fifty-nine patients (76.9 ± 6.3 years; 51% female) were included. The fracture was caused by a low-energy trauma mechanism in 22 patients (35.6%). Twenty-one patients died during the follow-up period (35.6%). Remaining patients (n = 38) were followed up after a mean of 60 months. Patients who died were significantly older (p = 0.01) and had significantly higher ASA scores (p = 0.02). Adjacent thoracic cage fractures had no effect on mortality or outcome scores. A total of 12 sequential vertebral fractures occurred (35.3%). The mean ODI at the latest follow up was 31.3 ± 24.7, the mean regional sagittal loss of reduction was 5.1° (± 4.0). Patients treated with long segmental stabilization had a significantly lower rate of sequential vertebral fractures during follow-up (p = 0.03).
Conclusion: Unstable fractures of the midthoracic spine are associated with high rates of thoracic cage injuries. The mortality rate was rather high. The majority of the survivors had minimal to moderate disabilities. Thereby, patients treated with long segmental stabilization had a significantly lower rate of sequential vertebral body fractures during follow-up.
Keywords: Long segmental posterior stabilization; Midthoracic spine; Osteoporotic vertebral body fracture; Posterior stabilization; Thoracic cage injury.
Conflict of interest statement
C.-E. Heyde: Royalties: Medacta (Switzerland).
G. Osterhoff: Consultant for Medtronic.
The authors declare that they have no further competing interests.
Figures



Similar articles
-
Hybrid stabilization of unstable osteoporotic thoracolumbar vertebral body fractures: clinical and radiological outcome after a mean of 4 years.Eur Spine J. 2019 May;28(5):1130-1137. doi: 10.1007/s00586-019-05957-8. Epub 2019 Mar 21. Eur Spine J. 2019. PMID: 30900093
-
Comparison of combined posterior and anterior spondylodesis versus hybrid stabilization in unstable burst fractures at the thoracolumbar spine in patients between 60 and 70 years of age.Arch Orthop Trauma Surg. 2018 Oct;138(10):1407-1414. doi: 10.1007/s00402-018-2993-y. Epub 2018 Jul 14. Arch Orthop Trauma Surg. 2018. PMID: 30008109
-
Which anatomic structures are responsible for the reduction loss after hybrid stabilization of osteoporotic fractures of the thoracolumbar spine?BMC Musculoskelet Disord. 2020 Jan 29;21(1):54. doi: 10.1186/s12891-020-3065-3. BMC Musculoskelet Disord. 2020. PMID: 31996180 Free PMC article.
-
Biomechanics and clinical outcome after posterior stabilization of mid-thoracic vertebral body fractures: a systematic literature review.Eur J Trauma Emerg Surg. 2021 Oct;47(5):1389-1398. doi: 10.1007/s00068-020-01560-5. Epub 2020 Dec 2. Eur J Trauma Emerg Surg. 2021. PMID: 33263816 Free PMC article.
-
Traumatic Fractures of the Thoracic Spine.Z Orthop Unfall. 2021 Aug;159(4):373-382. doi: 10.1055/a-1144-3846. Epub 2020 May 11. Z Orthop Unfall. 2021. PMID: 32392598 Review. English, German.
Cited by
-
Effect of subsequent vertebral body fractures on the outcome after posterior stabilization of unstable geriatric fractures of the thoracolumbar spine.BMC Musculoskelet Disord. 2022 Dec 5;23(1):1064. doi: 10.1186/s12891-022-06031-z. BMC Musculoskelet Disord. 2022. PMID: 36471332 Free PMC article.
-
Biomechanical comparative analysis of conventional pedicle screws and cortical bone trajectory fixation in the lumbar spine: An in vitro and finite element study.Front Bioeng Biotechnol. 2023 Jan 19;11:1060059. doi: 10.3389/fbioe.2023.1060059. eCollection 2023. Front Bioeng Biotechnol. 2023. PMID: 36741751 Free PMC article.
-
Clinical Validation of Commercial AI Software for the Detection of Incidental Vertebral Compression Fractures in CT Scans of the Chest and Abdomen.Diagnostics (Basel). 2025 Jun 16;15(12):1530. doi: 10.3390/diagnostics15121530. Diagnostics (Basel). 2025. PMID: 40564850 Free PMC article.
-
Geriatric spine fractures - Demography, changing trends, challenges and special considerations: A narrative review.J Clin Orthop Trauma. 2023 Jun 29;43:102190. doi: 10.1016/j.jcot.2023.102190. eCollection 2023 Aug. J Clin Orthop Trauma. 2023. PMID: 37538298 Free PMC article.
-
Characteristics and outcomes of inpatients aged 85 and older with thoracolumbar vertebral fractures: impact on hospital stay and mortality.Eur Spine J. 2024 Dec;33(12):4504-4512. doi: 10.1007/s00586-024-08520-2. Epub 2024 Oct 22. Eur Spine J. 2024. PMID: 39436426
References
-
- Abdelgawaad AS, Ezzati A, Govindasamy R, Krajnovic B, Elnady B, Said GZ. Kyphoplasty for osteoporotic vertebral fractures with posterior wall injury. Spine J. 2017. 10.1016/j.spinee.2017.11.001. - PubMed
-
- Rong Z, Zhang F, Xiao J, Wang Z, Luo F, Zhang Z, et al. Application of cement-injectable Cannulated pedicle screw in treatment of osteoporotic thoracolumbar vertebral compression fracture (AO type a): a retrospective study of 28 cases. World Neurosurg. 2018;120:e247–e258. doi: 10.1016/j.wneu.2018.08.045. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
