

Back to simplicity: a four-marker blood cell score to quantify prognostically relevant myeloid cells in melanoma patients
- PMID: 33589521
- PMCID: PMC7887358
- DOI: 10.1136/jitc-2020-001167
Back to simplicity: a four-marker blood cell score to quantify prognostically relevant myeloid cells in melanoma patients
Abstract
Background: Myeloid-derived suppressor cells (MDSC), a cornerstone of cancer-related immunosuppression, influence response to therapy and disease outcomes in melanoma patients. Nevertheless, their quantification is far from being integrated into routine clinical practice mostly because of the complex and still evolving phenotypic signatures applied to define the cell subsets. Here, we used a multistep downsizing process to verify whether a core of few markers could be sufficient to capture the prognostic potential of myeloid cells in peripheral blood mononuclear cells (PBMC) of metastatic melanoma patients.
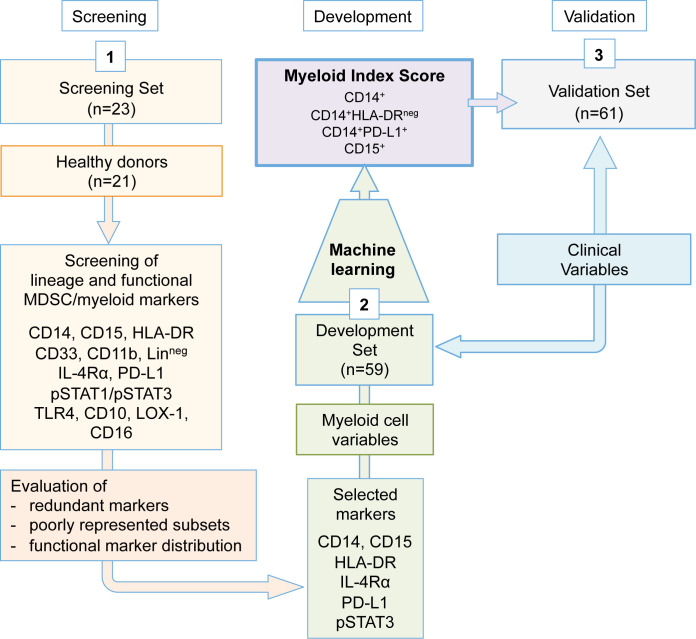
Methods: In baseline frozen PBMC from a total of 143 stage IIIc to IV melanoma patients, we first assessed the relevant or redundant expression of myeloid and MDSC-related markers by flow cytometry (screening set, n=23 patients). Subsequently, we applied the identified panel to the development set samples (n=59 patients undergoing first/second-line therapy) to obtain prognostic variables associated with overall survival (OS) and progression-free survival (PFS) by machine learning adaptive index modeling. Finally, the identified score was confirmed in a validation set (n=61) and compared with standard clinical prognostic factors to assess its additive value in patient prognostication.
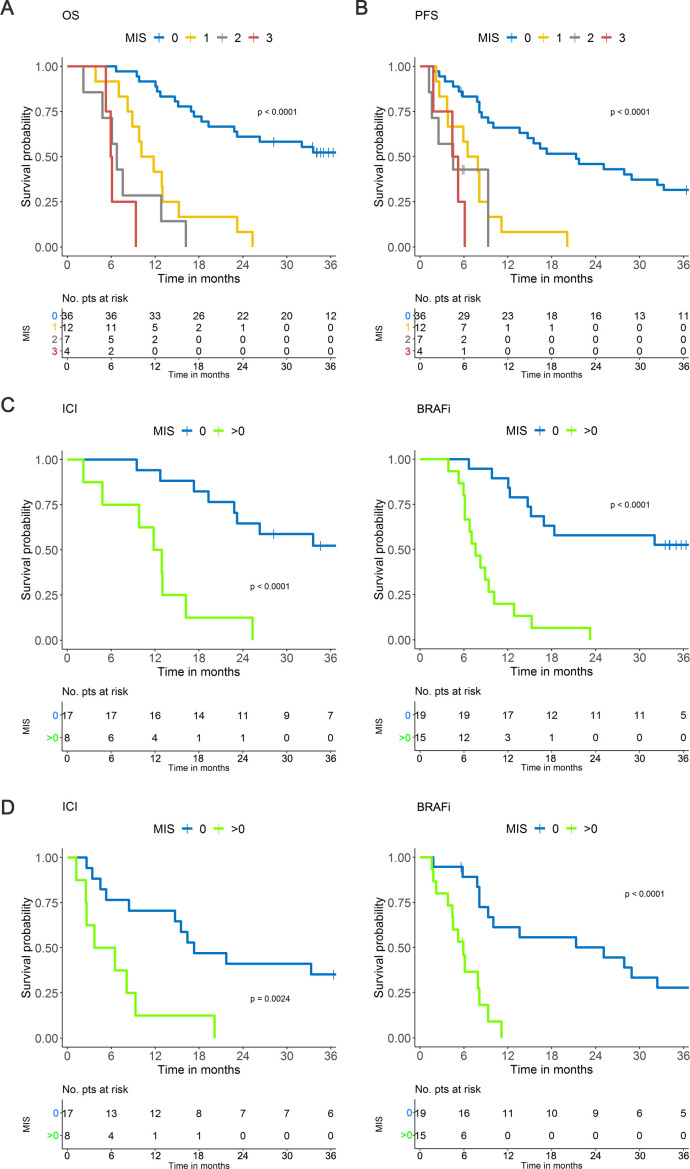
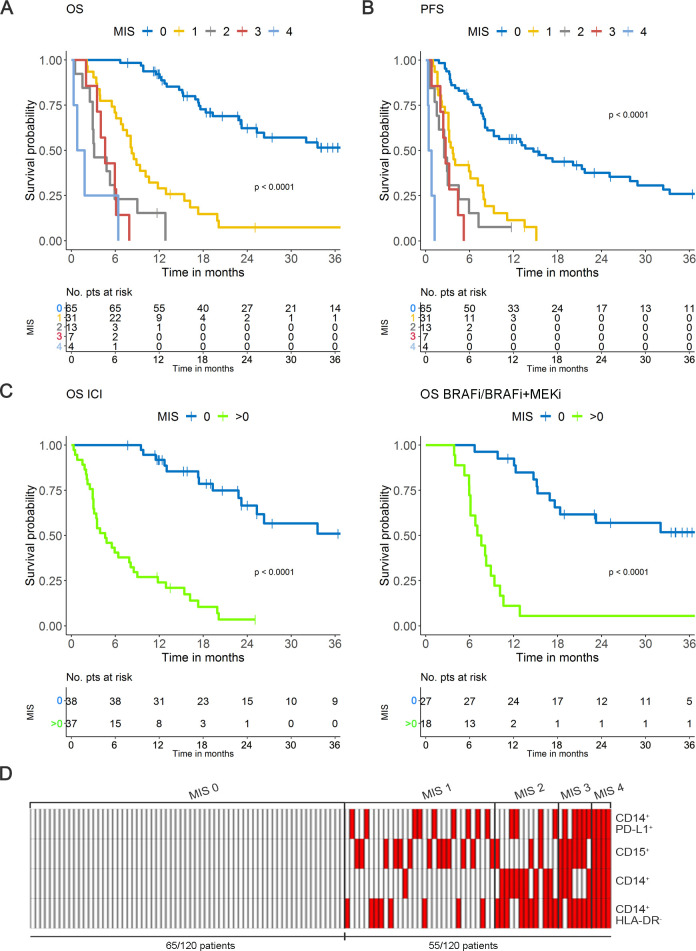
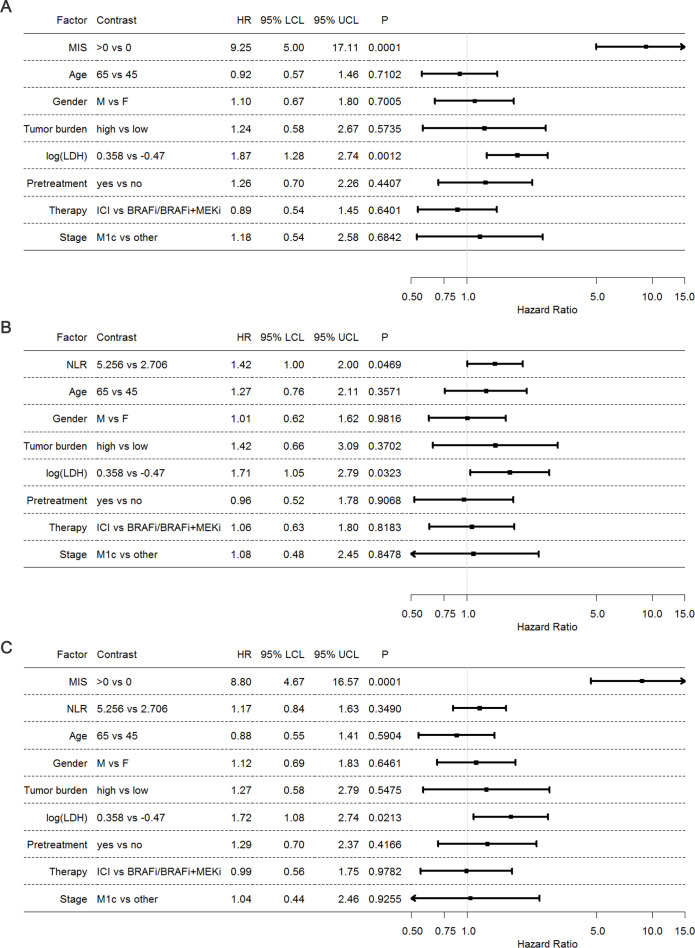
Results: This selection process led to the identification of what we defined myeloid index score (MIS), which is composed by four cell subsets (CD14+, CD14+HLA-DRneg, CD14+PD-L1+ and CD15+ cells), whose frequencies above cut-offs stratified melanoma patients according to progressively worse prognosis. Patients with a MIS=0, showing no over-threshold value of MIS subsets, had the best clinical outcome, with a median survival of >33.6 months, while in patients with MIS 1→3, OS deteriorated from 10.9 to 6.8 and 6.0 months as the MIS increased (p<0.0001, c-index=0.745). MIS clustered patients into risk groups also according to PFS (p<0.0001). The inverse correlation between MIS and survival was confirmed in the validation set, was independent of the type of therapy and was not interfered by clinical prognostic factors. MIS HR was remarkably superior to that of lactate dehydrogenase, tumor burden and neutrophil-to-lymphocyte ratio.
Conclusion: The MIS >0 identifies melanoma patients with a more aggressive disease, thus acting as a simple blood biomarker that can help tailoring therapeutic choices in real-life oncology.
Keywords: immune evasion; immunotherapy; melanoma; myeloid-derived suppressor cells; tumor biomarkers.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials