

Frequency and profile of objective cognitive deficits in hospitalized patients recovering from COVID-19
- PMID: 33589778
- PMCID: PMC7884062
- DOI: 10.1038/s41386-021-00978-8
Frequency and profile of objective cognitive deficits in hospitalized patients recovering from COVID-19
Abstract
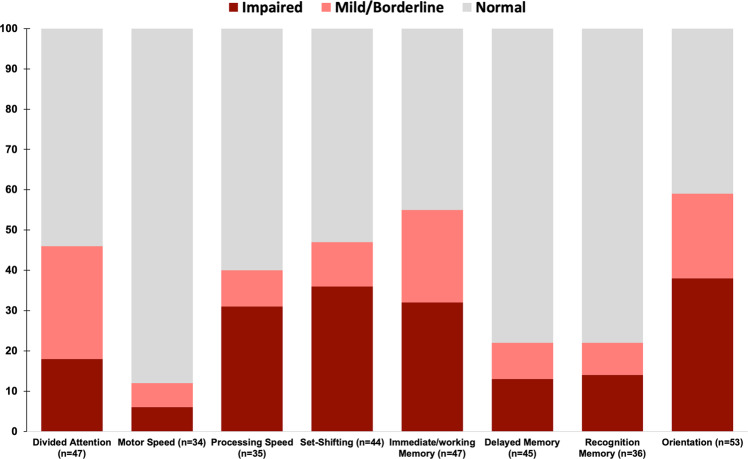
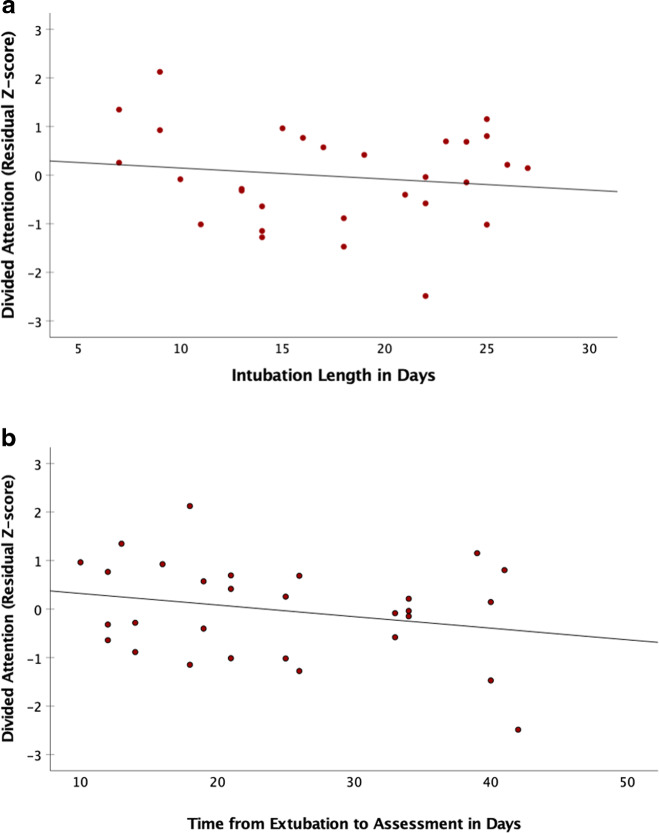
Early reports and case series suggest cognitive deficits occurs in some patients with COVID-19. We evaluated the frequency, severity, and profile of cognitive dysfunction in patients recovering from prolonged COVID-19 hospitalization who required acute inpatient rehabilitation prior to discharge. We analyzed cross-sectional scores from the Brief Memory and Executive Test (BMET) in a cohort of N = 57 COVID-19 patients undergoing inpatient rehabilitation, calculating the frequency of impairment based on neuropsychologist diagnosis and by age-normed BMET subtests. In total, 43 patients (75%) were male, 35 (61%) were non-white, and mean age was 64.5 (SD = 13.9) years. In total, 48 (84%) were previously living at home independently. Two patients had documented preexisting cognitive dysfunction; none had known dementia. Patients were evaluated at a mean of 43.2 (SD = 19.2) days after initial admission. In total, 50 patients (88%) had documented hypoxemic respiratory failure and 44 (77%) required intubation. Forty-six patients (81%) had cognitive impairment, ranging from mild to severe. Deficits were common in working memory (26/47 [55%] of patients), set-shifting (21/44 [47%]), divided attention (18/39 [46%]), and processing speed (14/35 [40%]). Executive dysfunction was not significantly associated with intubation length or the time from extubation to assessment, psychiatric diagnosis, or preexisting cardiovascular/metabolic disease. Attention and executive functions are frequently impaired in COVID-19 patients who require acute rehabilitation prior to discharge. Though interpretation is limited by lack of a comparator group, these results provide an early benchmark for identifying and characterizing cognitive difficulties after COVID-19. Given the frequency and pattern of impairment, easy-to-disseminate interventions that target attention and executive dysfunctions may be beneficial to this population.
© 2021. The Author(s), under exclusive licence to American College of Neuropsychopharmacology.
Figures
Comment in
-
The impact of COVID-19 on cognition in severe cases highlights the need for comprehensive neuropsychological evaluations in all survivors.Neuropsychopharmacology. 2021 Dec;46(13):2225. doi: 10.1038/s41386-021-00995-7. Epub 2021 Mar 22. Neuropsychopharmacology. 2021. PMID: 33753883 Free PMC article. No abstract available.
References
-
- Girard TD, Thompson JL, Pandharipande PP, Brummel NE, Jackson JC, Patel MB, et al. Clinical phenotypes of delirium during critical illness and severity of subsequent long-term cognitive impairment: a prospective cohort study. Lancet Respir Med. 2018;6:213–22. doi: 10.1016/S2213-2600(18)30062-6. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
