

Harnessing non-destructive 3D pathology
- PMID: 33589781
- PMCID: PMC8118147
- DOI: 10.1038/s41551-020-00681-x
Harnessing non-destructive 3D pathology
Abstract
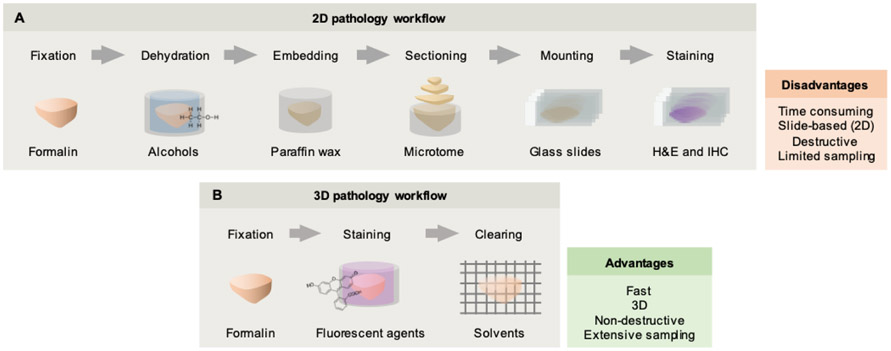
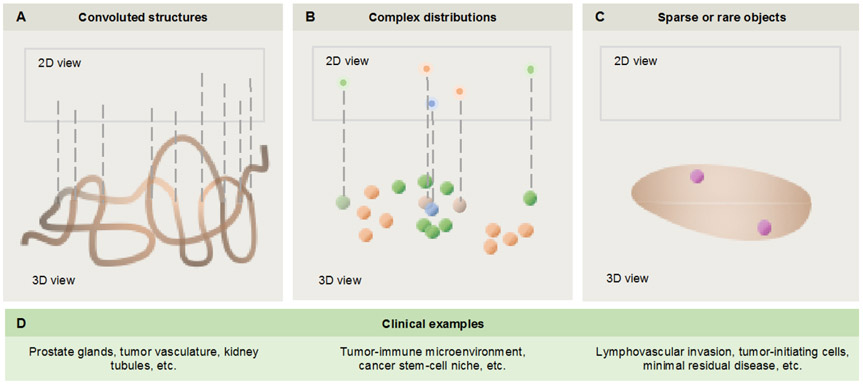
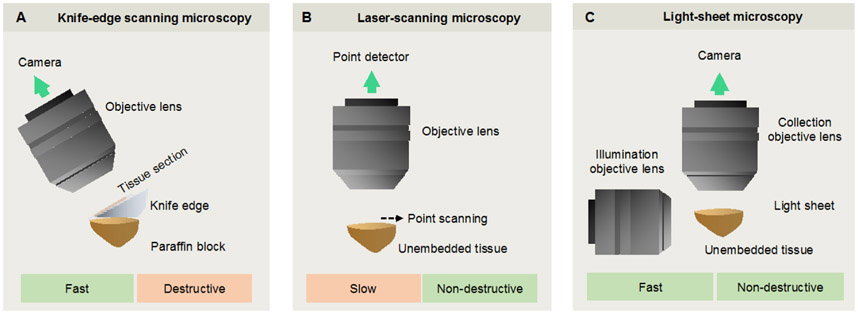
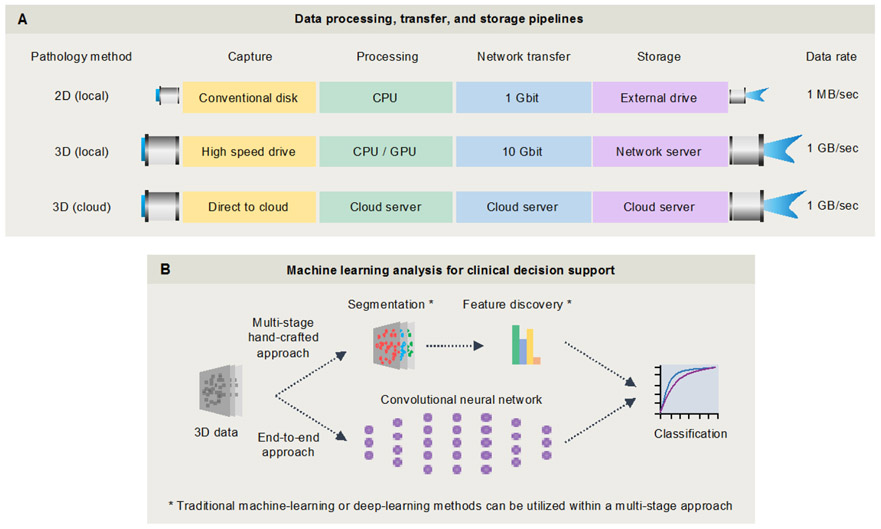
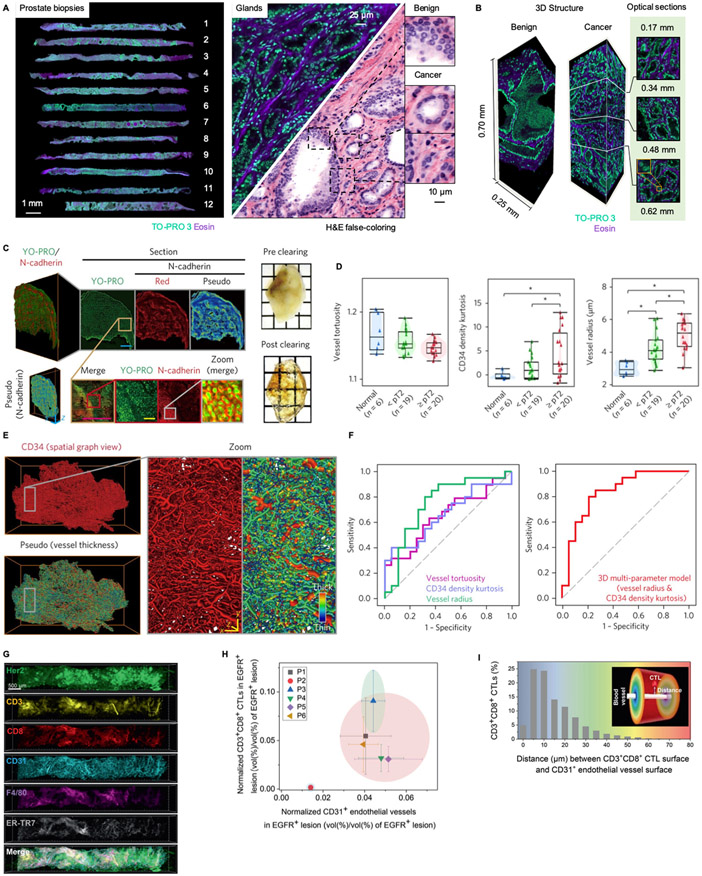
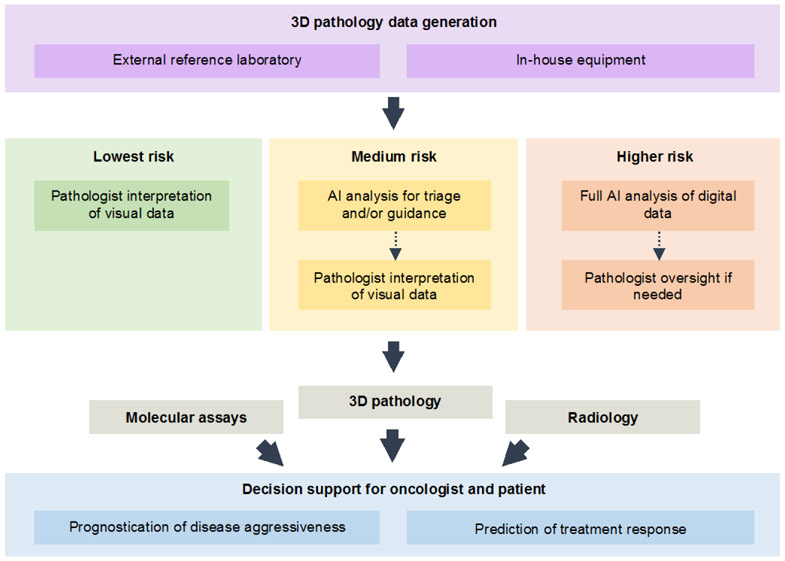
High-throughput methods for slide-free three-dimensional (3D) pathological analyses of whole biopsies and surgical specimens offer the promise of modernizing traditional histology workflows and delivering improvements in diagnostic performance. Advanced optical methods now enable the interrogation of orders of magnitude more tissue than previously possible, where volumetric imaging allows for enhanced quantitative analyses of cell distributions and tissue structures that are prognostic and predictive. Non-destructive imaging processes can simplify laboratory workflows, potentially reducing costs, and can ensure that samples are available for subsequent molecular assays. However, the large size of the feature-rich datasets that they generate poses challenges for data management and computer-aided analysis. In this Perspective, we provide an overview of the imaging technologies that enable 3D pathology, and the computational tools-machine learning, in particular-for image processing and interpretation. We also discuss the integration of various other diagnostic modalities with 3D pathology, along with the challenges and opportunities for clinical adoption and regulatory approval.
Figures
References
-
- Gradishar WJ, et al. NCCN Guidelines Insights Breast Cancer, Version 1.2016. J Natl Compr Canc Netw 13, 1475–1485 (2015). - PubMed
-
- McKenney JK, et al. The potential impact of reproducibility of Gleason grading in men with early stage prostate cancer managed by active surveillance: a multi-institutional study. in J Urol, Vol. 186 465–469 (2011). - PubMed
-
- Shah RB, et al. Diagnosis of Gleason pattern 5 prostate adenocarcinoma on core needle biopsy: an interobserver reproducibility study among urologic pathologists. in Am J Surg Pathol, Vol. 39 1242–1249 (2015). - PubMed
-
- Zhou M, et al. Diagnosis of "Poorly Formed Glands" Gleason Pattern 4 Prostatic Adenocarcinoma on Needle Biopsy: An Interobserver Reproducibility Study Among Urologic Pathologists With Recommendations. in Am J Surg Pathol, Vol. 39 1331–1339 (2015). - PubMed
Publication types
MeSH terms
Grants and funding
- R01 CA175391/CA/NCI NIH HHS/United States
- R01 CA244170/CA/NCI NIH HHS/United States
- R01 HL151277/HL/NHLBI NIH HHS/United States
- R01 CA216579/CA/NCI NIH HHS/United States
- R01 CA199996/CA/NCI NIH HHS/United States
- C06 RR012463/RR/NCRR NIH HHS/United States
- U24 CA199374/CA/NCI NIH HHS/United States
- K99 CA240681/CA/NCI NIH HHS/United States
- R43 EB028736/EB/NIBIB NIH HHS/United States
- U01 CA239055/CA/NCI NIH HHS/United States
- P41 GM135019/GM/NIGMS NIH HHS/United States
- R01 CA202752/CA/NCI NIH HHS/United States
- R01 CA208236/CA/NCI NIH HHS/United States
- U01 CA248226/CA/NCI NIH HHS/United States
- R00 CA240681/CA/NCI NIH HHS/United States
- U54 CA254566/CA/NCI NIH HHS/United States
- I01 BX004121/BX/BLRD VA/United States
- R01 CA220581/CA/NCI NIH HHS/United States
- R01 CA249992/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
