

Humoral signatures of protective and pathological SARS-CoV-2 infection in children
- PMID: 33589825
- PMCID: PMC8315827
- DOI: 10.1038/s41591-021-01263-3
Humoral signatures of protective and pathological SARS-CoV-2 infection in children
Abstract
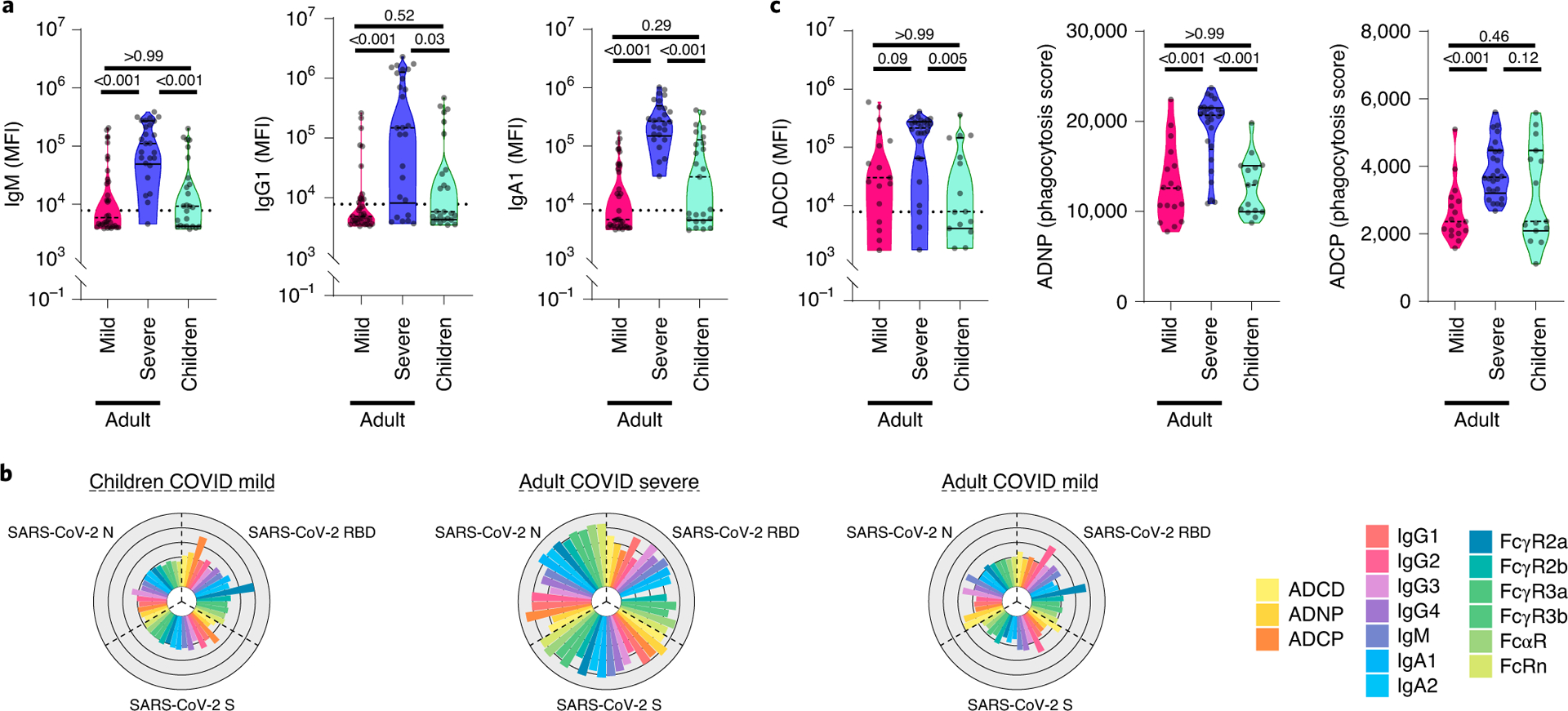
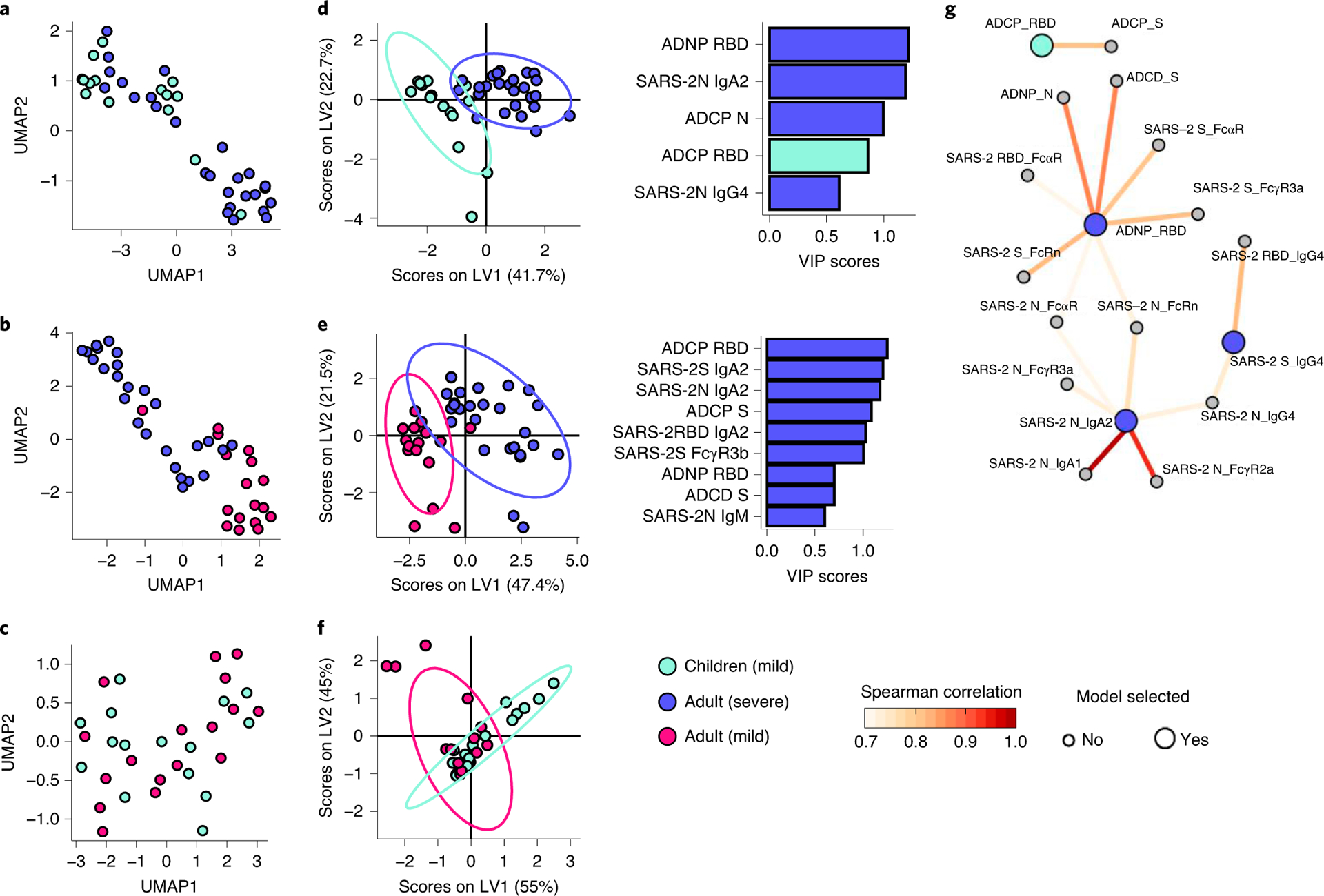
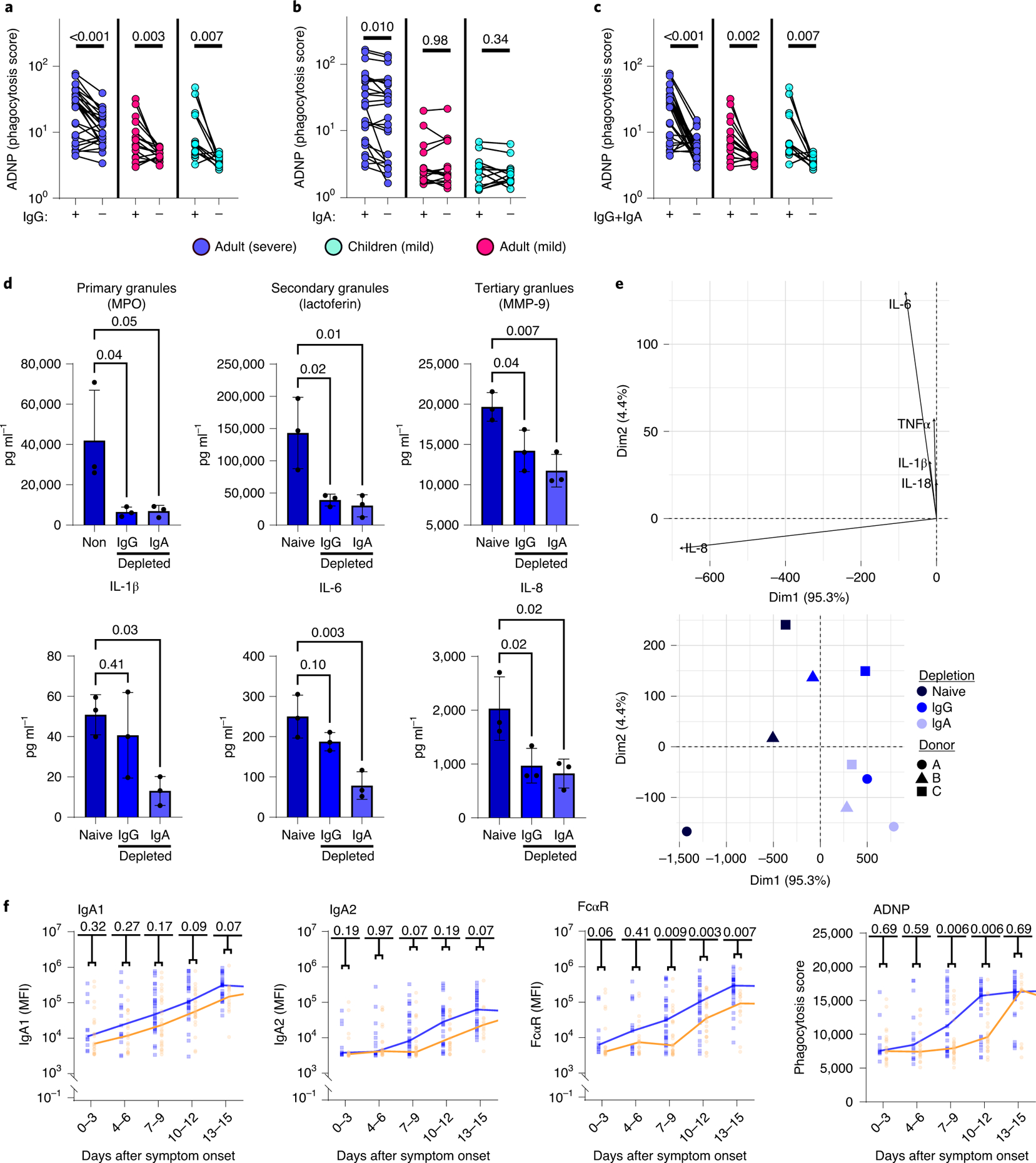
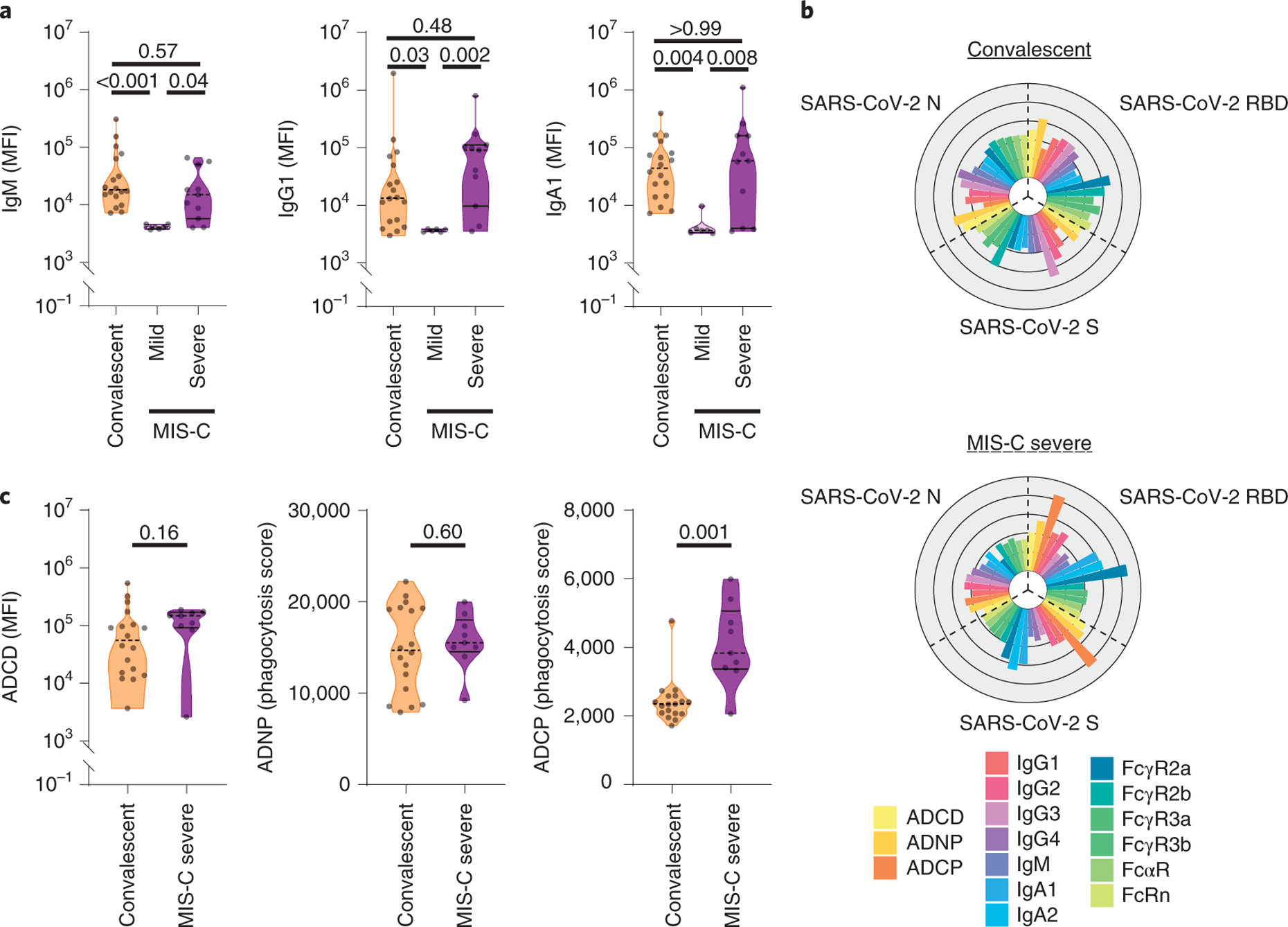
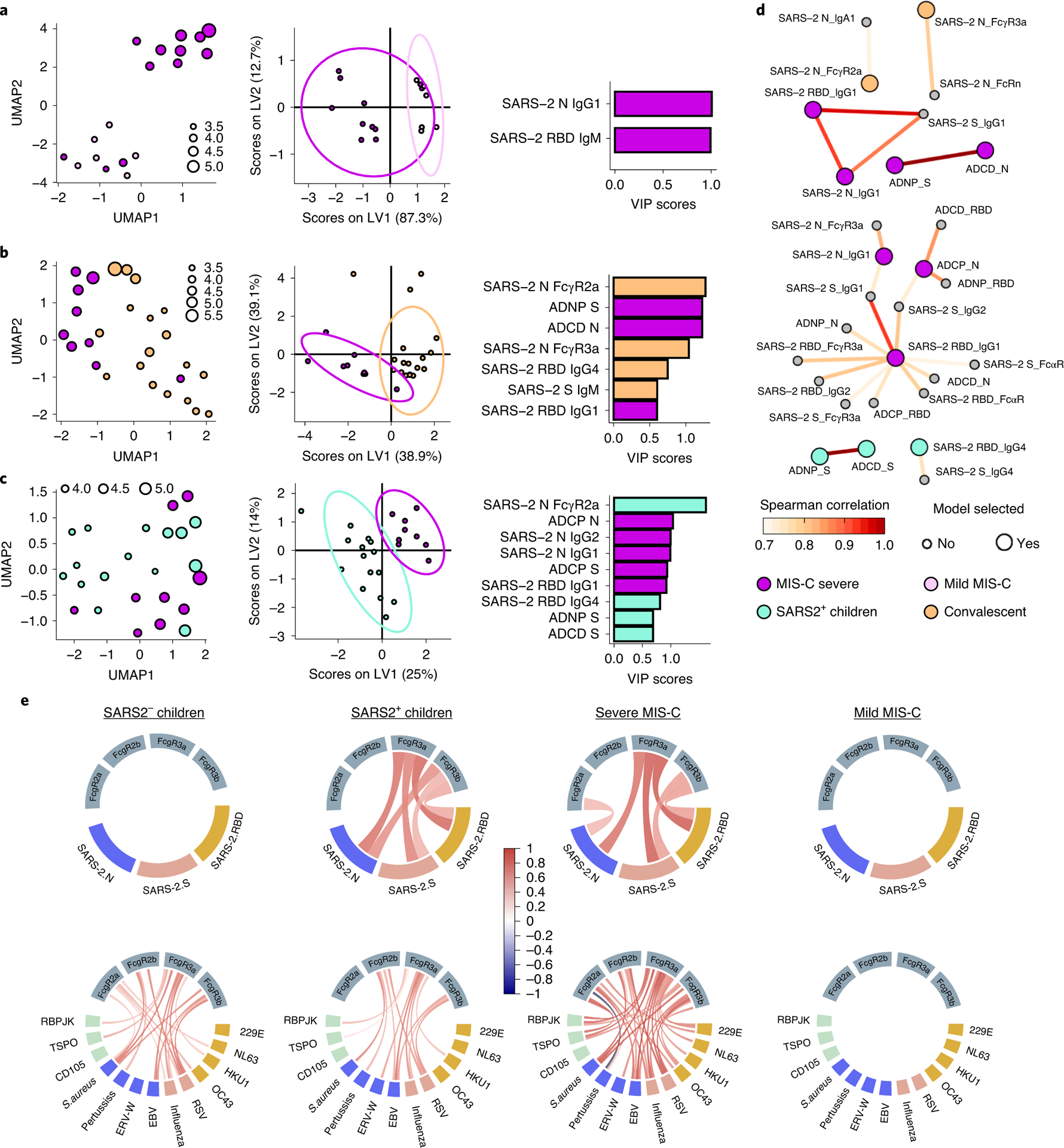
The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) pandemic continues to spread relentlessly, associated with a high frequency of respiratory failure and mortality. Children experience largely asymptomatic disease, with rare reports of multisystem inflammatory syndrome in children (MIS-C). Identifying immune mechanisms that result in these disparate clinical phenotypes in children could provide critical insights into coronavirus disease 2019 (COVID-19) pathogenesis. Using systems serology, in this study we observed in 25 children with acute mild COVID-19 a functional phagocyte and complement-activating IgG response to SARS-CoV-2, similar to the acute responses generated in adults with mild disease. Conversely, IgA and neutrophil responses were significantly expanded in adults with severe disease. Moreover, weeks after the resolution of SARS-CoV-2 infection, children who develop MIS-C maintained highly inflammatory monocyte-activating SARS-CoV-2 IgG antibodies, distinguishable from acute disease in children but with antibody levels similar to those in convalescent adults. Collectively, these data provide unique insights into the potential mechanisms of IgG and IgA that might underlie differential disease severity as well as unexpected complications in children infected with SARS-CoV-2.
Conflict of interest statement
Conflict of interest
Galit Alter is a founder of Seromyx Systems Inc, a company developing platform technology that describes the antibody immune response. Dr. Alter’s interests were reviewed and are managed by Massachusetts General Hospital and Partners HealthCare in accordance with their conflict of interest policies. All other authors have declared that no conflict of interest exists.
Figures
References
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
- 3R37AI080289-11S1/U.S. Department of Health & Human Services | National Institutes of Health (NIH)
- YONKER18Q0/Cystic Fibrosis Foundation (CF Foundation)
- U19 AI142790/AI/NIAID NIH HHS/United States
- R01 AI146779/AI/NIAID NIH HHS/United States
- U01 CK000490/CK/NCEZID CDC HHS/United States
- U01CK000490/ACL/ACL HHS/United States
- R01 GM092804/GM/NIGMS NIH HHS/United States
- 5K08HL143183/U.S. Department of Health & Human Services | NIH | National Heart, Lung, and Blood Institute (NHLBI)
- U01CK0009490/U.S. Department of Health & Human Services | Centers for Disease Control and Prevention (CDC)
- Global Health Vaccine Accelerator Platform/Bill and Melinda Gates Foundation (Bill & Melinda Gates Foundation)
- R01 HD100022/HD/NICHD NIH HHS/United States
- U19 AI135995/AI/NIAID NIH HHS/United States
- U01 CA260476/CA/NCI NIH HHS/United States
- R37 AI080289/AI/NIAID NIH HHS/United States
- K08 HL143183/HL/NHLBI NIH HHS/United States
- U01CA260476/U.S. Department of Health & Human Services | National Institutes of Health (NIH)
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
