

Potential intestinal infection and faecal-oral transmission of SARS-CoV-2
- PMID: 33589829
- PMCID: PMC7883337
- DOI: 10.1038/s41575-021-00416-6
Potential intestinal infection and faecal-oral transmission of SARS-CoV-2
Abstract
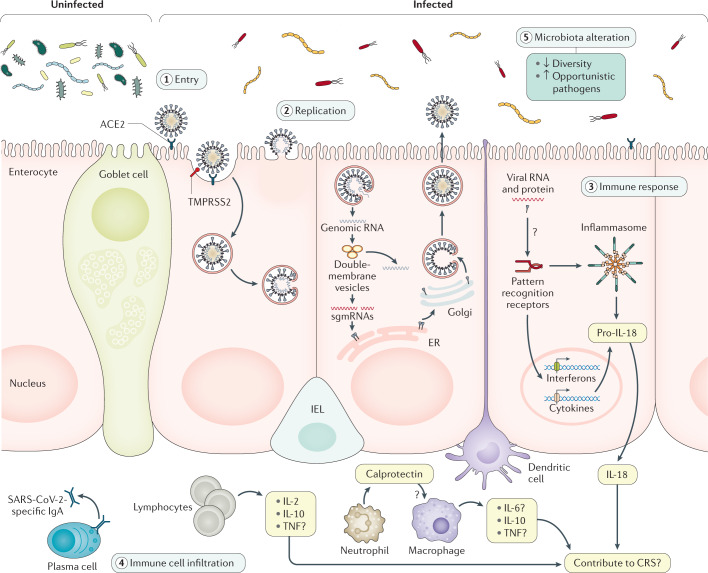
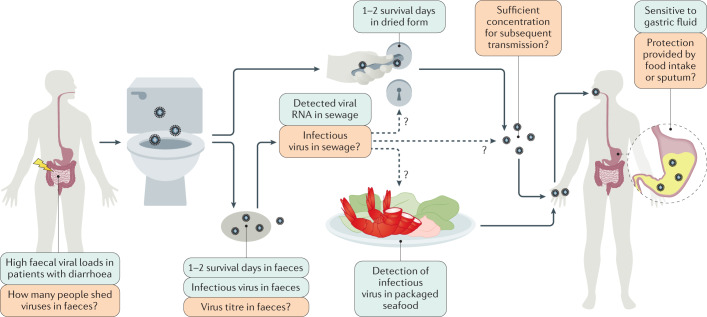
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has spread to more than 200 countries and regions globally. SARS-CoV-2 is thought to spread mainly through respiratory droplets and close contact. However, reports have shown that a notable proportion of patients with coronavirus disease 2019 (COVID-19) develop gastrointestinal symptoms and nearly half of patients confirmed to have COVID-19 have shown detectable SARS-CoV-2 RNA in their faecal samples. Moreover, SARS-CoV-2 infection reportedly alters intestinal microbiota, which correlated with the expression of inflammatory factors. Furthermore, multiple in vitro and in vivo animal studies have provided direct evidence of intestinal infection by SARS-CoV-2. These lines of evidence highlight the nature of SARS-CoV-2 gastrointestinal infection and its potential faecal-oral transmission. Here, we summarize the current findings on the gastrointestinal manifestations of COVID-19 and its possible mechanisms. We also discuss how SARS-CoV-2 gastrointestinal infection might occur and the current evidence and future studies needed to establish the occurrence of faecal-oral transmission.
Conflict of interest statement
The authors declare no competing interests.
Figures
Comment in
-
Rectally shed SARS-CoV-2 lacks infectivity: time to rethink faecal-oral transmission?Nat Rev Gastroenterol Hepatol. 2021 Sep;18(9):669. doi: 10.1038/s41575-021-00501-w. Nat Rev Gastroenterol Hepatol. 2021. PMID: 34312524 Free PMC article. No abstract available.
-
Reply to: Rectally shed SARS-CoV-2 lacks infectivity: time to rethink faecal-oral transmission?Nat Rev Gastroenterol Hepatol. 2021 Sep;18(9):669-670. doi: 10.1038/s41575-021-00503-8. Nat Rev Gastroenterol Hepatol. 2021. PMID: 34312525 Free PMC article. No abstract available.
References
-
- WHO. WHO coronavirus disease (COVID-19) dashboard. WHOhttps://covid19.who.int/ (2020).
-
- Lan J, et al. Structure of the SARS-CoV-2 spike receptor-binding domain bound to the ACE2 receptor. Nature. 2020;581:215–220. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
