

Disease burden and economic impact of diagnosed non-alcoholic steatohepatitis in five European countries in 2018: A cost-of-illness analysis
- PMID: 33590598
- PMCID: PMC8252761
- DOI: 10.1111/liv.14825
Disease burden and economic impact of diagnosed non-alcoholic steatohepatitis in five European countries in 2018: A cost-of-illness analysis
Abstract
Background and aims: Non-alcoholic steatohepatitis (NASH) is a chronic disease that can progress to end-stage liver disease (ESLD). A large proportion of early-stage NASH patients remain undiagnosed compared to those with advanced fibrosis, who are more likely to receive disease management interventions. This study estimated the disease burden and economic impact of diagnosed NASH in the adult population of France, Germany, Italy, Spain and the United Kingdom in 2018.
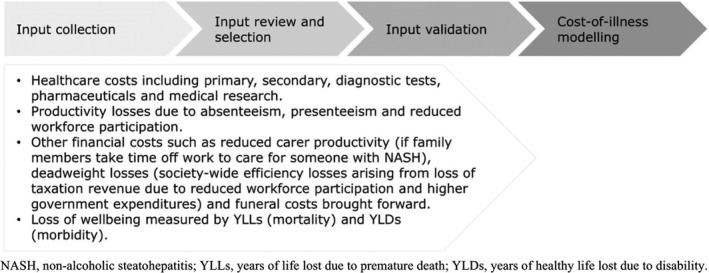
Methods: The socioeconomic burden of diagnosed NASH was estimated using cost-of-illness methodology applying a prevalence approach to estimate the number of adults with NASH and the attributable economic and wellbeing costs. Given undiagnosed patients do not incur costs in the study, the probability of diagnosis is central to cost estimation. The analysis was based on a literature review, databases and consultation with clinical experts, economists and patient groups.
Results: The proportion of adult NASH patients with a diagnosis ranged from 11.9% to 12.7% across countries, which increased to 38.8%-39.1% for advanced fibrosis (F3-F4 compensated cirrhosis). Total economic costs were €8548-19 546M. Of these, health system costs were €619-1292M. Total wellbeing costs were €41 536-90 379M. The majority of the undiagnosed population (87.3%-88.2% of total prevalence) was found to have early-stage NASH, which, left untreated, may progress to more resource consuming ESLD over time.
Conclusions: This study found that the majority of economic and wellbeing costs of NASH are experienced in late disease stages. Earlier diagnosis and care of NASH patients could reduce future healthcare costs.
Keywords: burden of disease; cost-of-illness analysis; economic impact; healthcare resource utilisation; non-alcoholic steatohepatitis (NASH).
© 2021 The Authors. Liver International published by John Wiley & Sons Ltd.
Conflict of interest statement
Alice Morgan, Sally L Sansom, Sharad Vasudevan and Lynne Pezzullo have received funding from Intercept Pharmaceuticals for consulting services. Jörn Schattenberg reports grants and personal fees from Gilead Sciences; and personal fees from Genfit, Intercept Pharmaceuticals, IQVIA, Novartis, Roche, Bristol‐Myers Squibb and Echosens, outside the submitted work. Jeffrey Lazarus reports personal fees from CEPHEID, GSK and Janssen; grants, personal fees and other from Abbvie and Gilead Sciences; and grants and personal fees from MSD, outside the submitted work. Philip N Newsome reports grants from Novo Nordisk and Boehringer Ingelheim; and other fees from Novo Nordisk, Pfizer, Boehringer Ingelheim, Intercept Pharmaceuticals, Gilead Sciences and Poxel Pharmaceuticals, outside the submitted work. Philip N Newsome is also supported by the National Institute for Health Research (NIHR) Birmingham Biomedical Research Centre at the University Hospitals Birmingham NHS Foundation Trust and the University of Birmingham. The views expressed are those of the author and not necessarily those of the NIHR, the Department of Health and Social Care or the NHS. Lawrence Serfaty reports grants and personal fees from Gilead Sciences; and personal fees from Intercept Pharmaceuticals, AbbVie, Novartis and Pfizer, outside the submitted work. Alessio Aghemo reports grant and research support from AbbVie and Gilead Sciences; and personal fees from MSD, Intercept Pharmaceuticals and AlfaSigma, outside the submitted work. Salvador Augustin reports personal fees from Intercept Pharmaceuticals as part of the submitted work. Salvador Augustin also reports grants and personal fees from Gilead Sciences; and personal fees from Novartis, Pfizer, IQVIA and Allergan, outside the submitted work. Emmanuel Tsochatzis reports personal fees from Intercept Pharmaceuticals, Gilead Sciences and Pfizer, outside the submitted work. Victor de Ledinghen reports grants and non‐financial support from Gilead, AbbVie and Intercept Pharmaceuticals; and personal fees from Gilead, AbbVie, Intercept Pharmaceuticals, Echosens, Supersonic Image, Pfizer, Medac, Indivior, Spimaco, BMS, Bayer and MSD, outside the submitted work. Elisabetta Bugianesi has no conflicts of interest to disclose. Manuel Romero‐Gomez reports grants from AbbVie, Gilead Sciences and Intercept Pharmaceuticals; is a speaker for Gilead Sciences, Intercept Pharmaceuticals, Novo Nordisk, Novartis and Shionogi; is a scientific advisor for Gilead Sciences, Intercept Pharmaceuticals, Novo Nordisk, Prosciento, Kaleido, Boehringer Ingelheim, BMS, Shionogi and Allergan; and is co‐owner of DeMILI, outside the submitted work. Heike Bantel reports personal fees from Intercept Pharmaceuticals, outside the submitted work. Stephen Ryder has attended advisory boards and acted as a paid speaker for Intercept Pharmaceuticals, outside the submitted work. Jerome Boursier has no conflicts of interest to disclose. Javier Crespo reports grant, consultancy and lecture fees from AbbVie, Gilead Sciences, Intercept Pharmaceuticals and MSD. Laurent Castera reports personal fees from AbbVie, Allergan, Echosens, Gilead Sciences, Intercept Pharmaceuticals, Merck, Novo Nordisk, Pfizer and Servier as part of the submitted work. Lefteris Floros has no conflicts of interests to report. Vincenzo Atella has no conflicts of interest to disclose. Jorge Mestre‐Ferrandiz reports personal fees form Intercept Pharmaceuticals as part of the submitted work. Rachel Elliot has no conflicts of interest to disclose. Achim Kautz has no conflicts of interest to disclose. Vlad Ratziu reports other fees from Intercept Pharmaceuticals, outside the submitted work. Victoria Higgins is an employee of Adelphi Real World who have received funding from Intercept Pharmaceuticals for access to the Adelphi NASH DSP data. Aldo Tyrelsinski and Sandrine Cure have received consultancy fees from, and are current employees of, Intercept Pharmaceuticals.
Figures
References
-
- Chalasani N, Younossi Z, Lavine JE, et al. The diagnosis and management of non‐alcoholic fatty liver disease: practice guideline by the American Gastroenterological Association, American Association for the Study of Liver Diseases, and American College of Gastroenterology. Gastroenterology. 2012;142(7):1592‐1609. - PubMed
-
- Younossi ZM, Blissett D, Blissett R, et al. The economic and clinical burden of non‐alcoholic fatty liver disease in the United States and Europe. Hepatology. 2016;64(5):1577‐1586. - PubMed
-
- Loomba R, Sanyal AJ. The global NAFLD epidemic. Nat Rev Gastroenterol Hepatol. 2013;10(11):686‐690. - PubMed
-
- Estes C, Anstee QM, Arias‐Loste MT, et al. Modeling NAFLD disease burden in China, France, Germany, Italy, Japan, Spain, United Kingdom, and United States for the period 2016–2030. J Hepatol. 2018;69(4):896‐904. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
