

A novel tissue inhibitor of metalloproteinases-1/liver/cachexia score predicts prognosis of gastrointestinal cancer patients
- PMID: 33590974
- PMCID: PMC8061407
- DOI: 10.1002/jcsm.12680
A novel tissue inhibitor of metalloproteinases-1/liver/cachexia score predicts prognosis of gastrointestinal cancer patients
Abstract
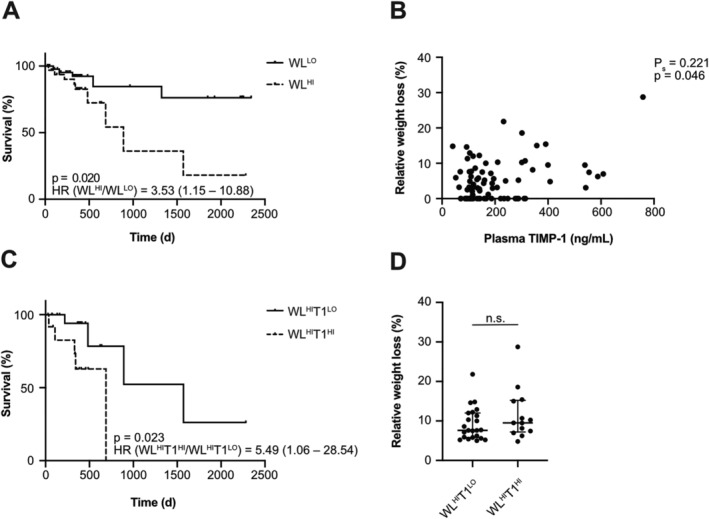
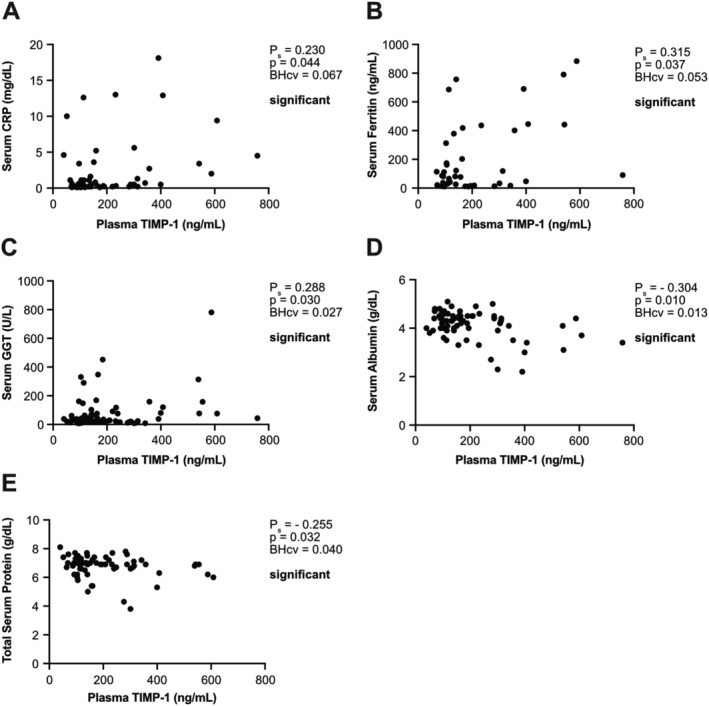
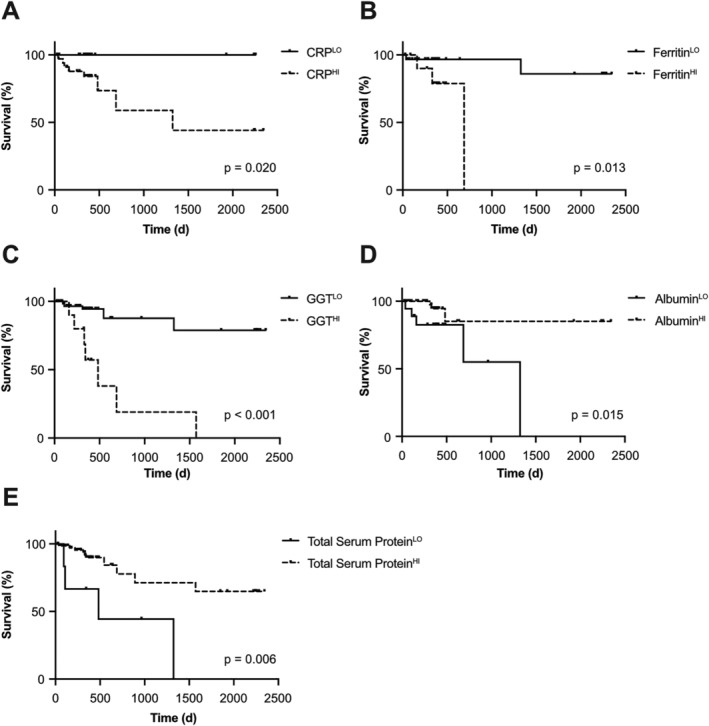
Background: Cachexia, a devastating syndrome in cancer patients, critically determines survival and life quality. It is characterized by impaired homeostasis of multiple organs including the liver, involves tissue wasting, and is conventionally diagnosed and classified by weight loss (WL). However, recent studies pointed at the problem that WL is not sufficient for precise classification of cancer patients according to disease severity (i.e. prognosis). Tissue inhibitor of metalloproteinases-1 (TIMP-1) is an easily accessible cachexia-associated biomarker in the blood, known to alter liver homeostasis. Here, we investigated the value of combining blood levels of TIMP-1 with parameters of liver functionality towards establishment of a cachexia-associated clinical score, which predicts survival of cancer patients, reflects the clinical manifestation of cachexia, and is easily accessible in the clinic.
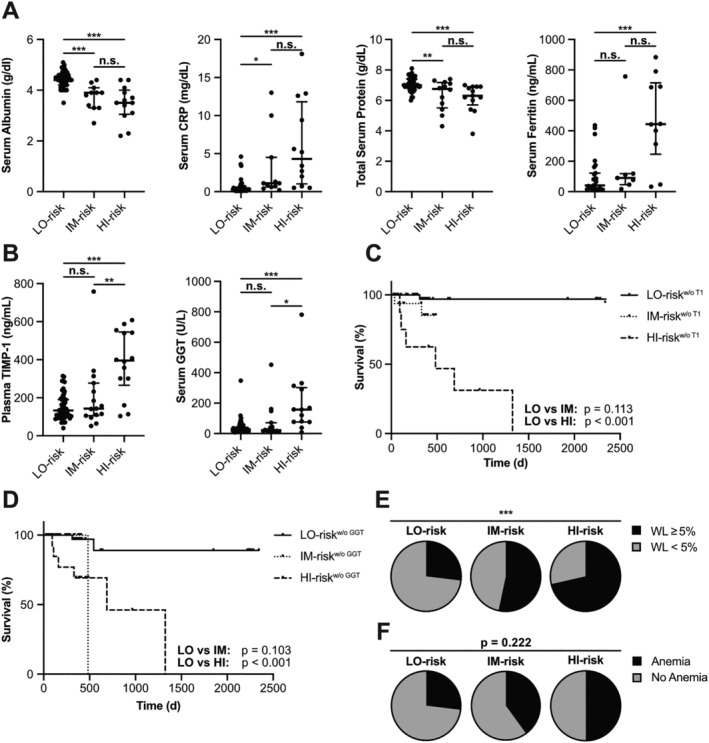
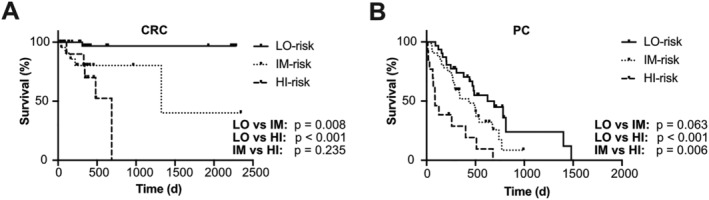
Methods: The TIMP-1/liver cachexia (TLC) score, expressed as numerical value ranging from 0 to 1, was calculated by categorizing the blood levels of TIMP-1 and parameters of liver functionality (C-reactive protein, ferritin, gamma-glutamyl transferase, albumin, and total protein) for each patient as below/above a certain risk threshold. The TLC score was tested in a cohort of colorectal cancer (CRC) patients (n = 82, 35.4% women, 64.6% men, median age: 70 years) and validated in a cohort of pancreatic cancer (PC) patients (n = 84, 54.8% women, 45.2% men, median age: 69 years).
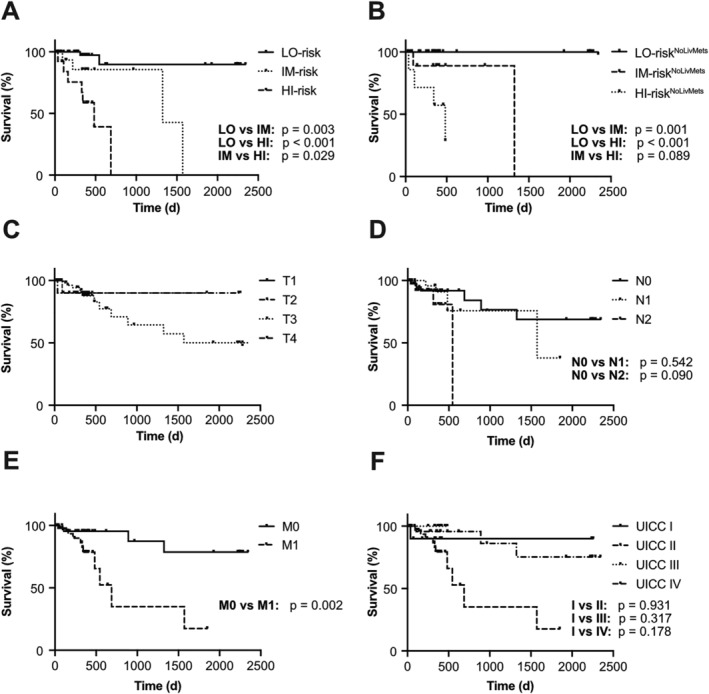
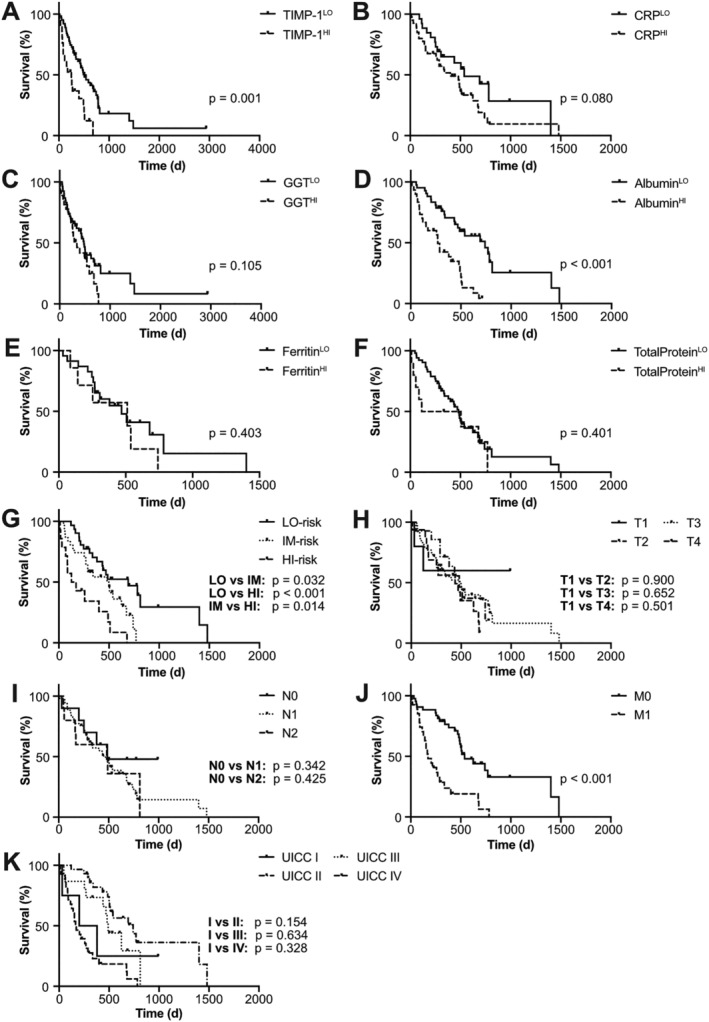
Results: In CRC patients, the TLC score positively correlated with presence of cachexia-related symptoms (WL, impaired liver function), predicted survival [P < 0.001, hazard ratio (HR): 96.91 (9.85-953.90)], and allowed classification of three prognostically distinct patient subpopulations [low (LO)-risk, intermediate (IM)-risk, and high (HI)-risk groups; LO vs. IM: P = 0.003, LO vs. HI: P < 0.001, IM vs. HI: P = 0.029]. The prognostic power of the cachexia-associated TLC score [P < 0.001, HR: 7.37 (2.80-19.49)] and its application to define risk groups (LO vs. IM: P = 0.032, LO vs. HI: P < 0.001, IM vs. HI: P = 0.014) was confirmed in a cohort of PC patients. The prognostic power of the TLC score was independent of presence of liver metastases in CRC or PC patients and was superior to clinically established staging classifications.
Conclusions: The TLC score, a result of straightforward determination of blood parameters, is an objective cachexia-associated clinical tool for precise survival prediction of gastrointestinal cancer patients.
Keywords: Cachexia; Gastrointestinal cancer; Prognostic score; TIMP-1.
© 2021 The Authors. Journal of Cachexia, Sarcopenia and Muscle published by John Wiley & Sons Ltd on behalf of the Society on Sarcopenia, Cachexia and Wasting Disorders.
Conflict of interest statement
The authors have no conflict of interest.
Figures
References
-
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2018;68:394–424. - PubMed
-
- Quaresma M, Coleman MP, Rachet B. 40‐year trends in an index of survival for all cancers combined and survival adjusted for age and sex for each cancer in England and Wales, 1971–2011: a population‐based study. The Lancet 2015;385:1206–1218. - PubMed
-
- Schmidt SF, Rohm M, Herzig S, Berriel Diaz M. Cancer cachexia: more than skeletal muscle wasting. Trends Cancer 2018;4:849–860. - PubMed
-
- Argiles JM, Stemmler B, Lopez‐Soriano FJ, Busquets S. Inter‐tissue communication in cancer cachexia. Nat Rev Endocrinol 2018;15:9–20. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
