

Admission Hemoglobin Levels Are Associated With Functional Outcome in Spontaneous Intracerebral Hemorrhage
- PMID: 33591003
- PMCID: PMC8611893
- DOI: 10.1097/CCM.0000000000004891
Admission Hemoglobin Levels Are Associated With Functional Outcome in Spontaneous Intracerebral Hemorrhage
Abstract
Objectives: To test the hypothesis that admission hemoglobin levels are associated with outcome in primary, nontraumatic intracerebral hemorrhage.
Design: Individual patient data meta-analysis of three studies of intracerebral hemorrhage.
Setting: Two randomized clinical trials and one multiethnic observational study.
Patients: Patients with spontaneous, nontraumatic intracerebral hemorrhage.
Interventions: None.
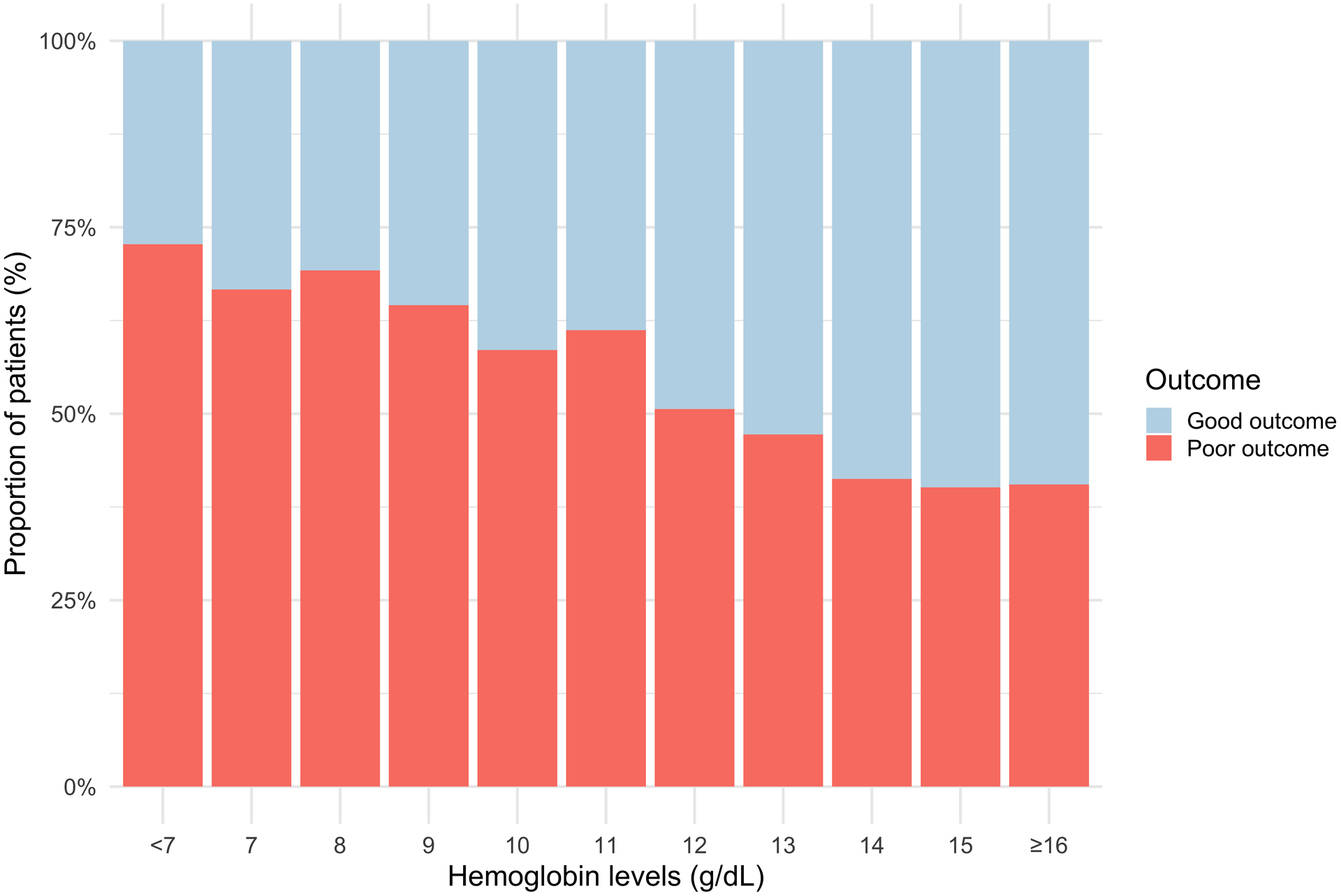
Measurements and main results: Our exposure of interest was admission hemoglobin levels and the primary outcome was 3-month postintracerebral hemorrhage-dichotomized modified Rankin Scale (0-3 vs 4-6). Intermediate outcomes were admission hematoma volume and hematoma expansion defined as 6 mL or 33% increase in hemorrhage size on repeat CT. A total of 4,172 intracerebral hemorrhage patients were included in the study (mean age 63 [sd = 14]; female sex 1,668 [40%]). Each additional g/dL of admission hemoglobin was associated with 14% (odds ratio, 0.86; 95% CI, 0.82-0.91) and 7% (odds ratio, 0.93; 95% CI, 0.88-0.98) reductions in the risk of poor outcome in unadjusted and adjusted analyses, respectively. Dose-response analyses indicated a linear relationship between admission hemoglobin levels and poor outcome across the entire evaluated range (test-for-trend p < 0.001). No consistent associations were found between the admission hemoglobin levels and hematoma volume or hematoma expansion.
Conclusions: Higher hemoglobin levels are associated with better outcome in intracerebral hemorrhage. Further research is needed to evaluate admission hemoglobin levels as both a therapeutic target and predictor of outcome.
Copyright © 2021 by the Society of Critical Care Medicine and Wolters Kluwer Health, Inc. All Rights Reserved.
Conflict of interest statement
Ms. Leasure is supported by the National Institutes of Health (NIH) (R03NS112859). Dr. Sansing is supported by the NIH (R01NS095993, R01NS097728, U01NS113445). Dr. Kamel is supported by the NIH (R01NS097443, U01NS095869, R01HL144541, U01NS106513). Dr. Murthy is supported by the NIH (K23NS105948) and the Leon Levy Foundation. Dr. Sheth is supported by the NIH (U24NS107136, U24NS107215, R01NR018335, U01NS106513, R03NS112859) and the American Heart Association (18TPA34170180,17CSA33550004). Dr. Falcone is supported by the National Institute on Aging (K76AG59992), the National Institute of Neurological Disorders and Stroke (R03NS112859), the American Heart Association (18IDDG34280056), a Yale Pepper Scholar Award (P30AG021342), and the Neurocritical Care Society Research Fellowship. Drs. Acosta, Sansing, Langefeld, Woo, Sheth, and Falcone received support for article research from the NIH. Drs. Langefeld’s and Woo’s institutions received funding from the NIH. Dr. Kamel serves as a principal investigator for the NIH-funded AtRial Cardiopathy and Antithrombotic Drugs In Prevention After Cryptogenic Stroke (ARCADIA) trial (National Institute of Nuerological Disoders and Stroke U01NS095869), which receives in-kind study drug from the Bristol-Myers-Squibb-Pfizer Alliance for Eliquis and ancillary study support from Roche Diagnostics, serves as Deputy Editor for JAMA Neurology, serves as a steering committee member of Medtronic’s Stroke atrial fibrillation trial (uncompensated), serves on an end point adjudication committee for a trial of empagliflozin for Boehringer-Ingelheim, and has served on an advisory board for Roivant Sciences related to Factor XI inhibition. Dr. Mayer recieved funding from Idorsia, MaxQ AI, Bayer, Brain Cool, Biogen, and Nestle. Dr. Sheth’s institution received funding from Biogen, Novartis, and Bard, and he recieved funding from Hyperfine and Zoll. The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
Comment in
-
[Neurosurgical intensive care medicine : Intensive medical care studies from 2020/2021].Anaesthesist. 2021 Sep;70(9):789-794. doi: 10.1007/s00101-021-00978-9. Epub 2021 Aug 10. Anaesthesist. 2021. PMID: 34378066 German. No abstract available.
-
Hemoglobin Level at Admission Is Less Important.Crit Care Med. 2022 Feb 1;50(2):e214-e215. doi: 10.1097/CCM.0000000000005323. Crit Care Med. 2022. PMID: 35100203 No abstract available.
-
The authors reply.Crit Care Med. 2022 Feb 1;50(2):e215-e216. doi: 10.1097/CCM.0000000000005388. Crit Care Med. 2022. PMID: 35100204 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
- R01 NR018335/NR/NINR NIH HHS/United States
- U24 NS107136/NS/NINDS NIH HHS/United States
- K76 AG059992/AG/NIA NIH HHS/United States
- P30 AG021342/AG/NIA NIH HHS/United States
- U24 NS107215/NS/NINDS NIH HHS/United States
- U01 NS113445/NS/NINDS NIH HHS/United States
- R01 HL144541/HL/NHLBI NIH HHS/United States
- R01 NS097728/NS/NINDS NIH HHS/United States
- R03 NS112859/NS/NINDS NIH HHS/United States
- R01 NS095993/NS/NINDS NIH HHS/United States
- R01 NS097443/NS/NINDS NIH HHS/United States
- U01 NS095869/NS/NINDS NIH HHS/United States
- U01 NS106513/NS/NINDS NIH HHS/United States
- K23 NS105948/NS/NINDS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
