

d-dimer and Death in Critically Ill Patients With Coronavirus Disease 2019
- PMID: 33591017
- PMCID: PMC8275993
- DOI: 10.1097/CCM.0000000000004917
d-dimer and Death in Critically Ill Patients With Coronavirus Disease 2019
Abstract
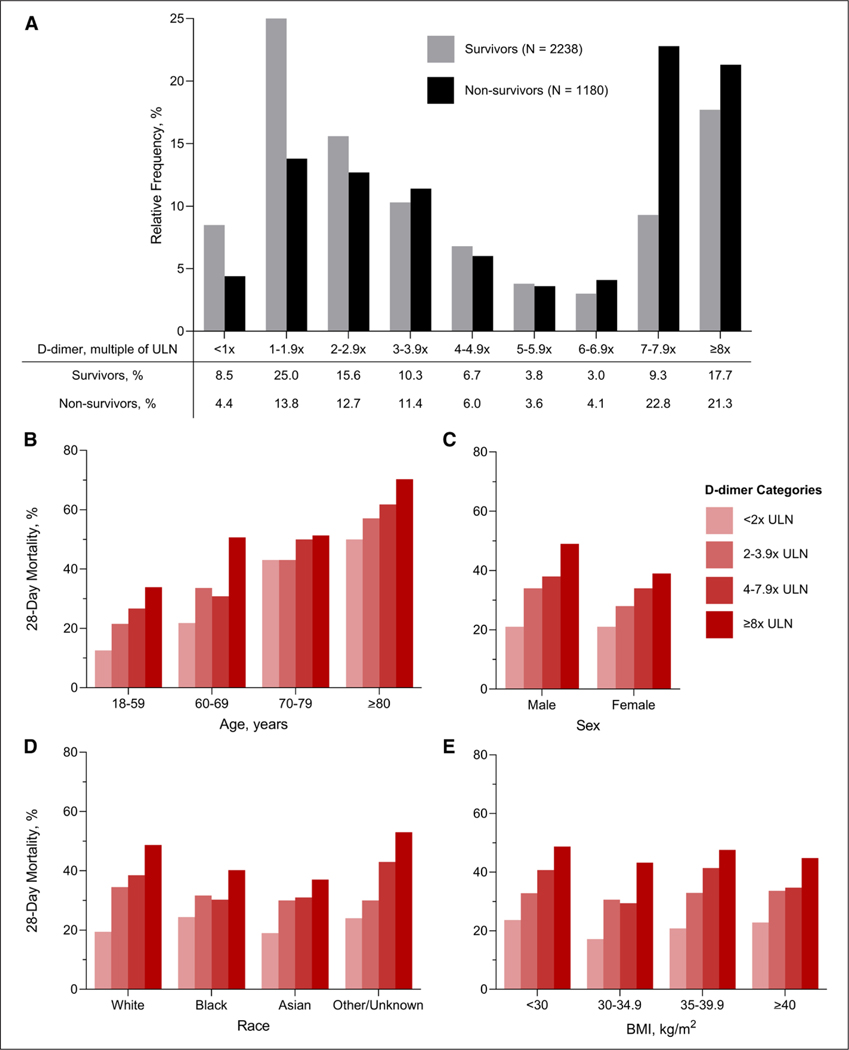
Objectives: Hypercoagulability may be a key mechanism for acute organ injury and death in patients with severe coronavirus disease 2019, but the relationship between elevated plasma levels of d-dimer, a biomarker of coagulation activation, and mortality has not been rigorously studied. We examined the independent association between d-dimer and death in critically ill patients with coronavirus disease 2019.
Design: Multicenter cohort study.
Setting: ICUs at 68 hospitals across the United States.
Patients: Critically ill adults with coronavirus disease 2019 admitted to ICUs between March 4, 2020, and May 25, 2020, with a measured d-dimer concentration on ICU day 1 or 2.
Interventions: None.
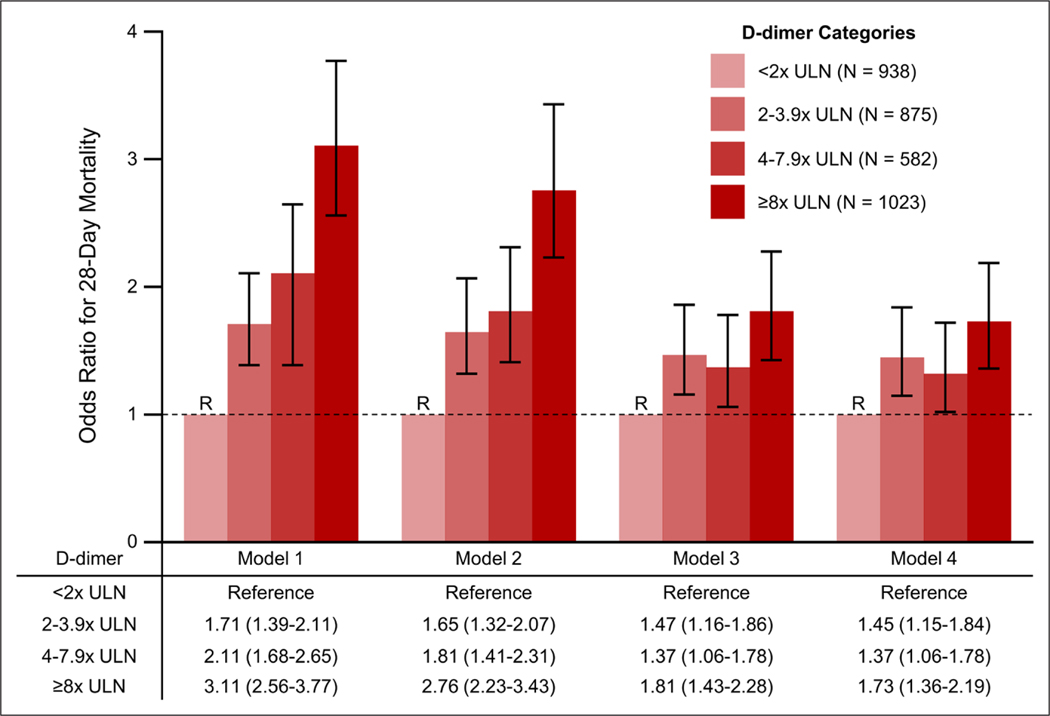
Measurements and main results: The primary exposure was the highest normalized d-dimer level (assessed in four categories: < 2×, 2-3.9×, 4-7.9×, and ≥ 8× the upper limit of normal) on ICU day 1 or 2. The primary endpoint was 28-day mortality. Multivariable logistic regression was used to adjust for confounders. Among 3,418 patients (63.1% male; median age 62 yr [interquartile range, 52-71 yr]), 3,352 (93.6%) had a d-dimer concentration above the upper limit of normal. A total of 1,180 patients (34.5%) died within 28 days. Patients in the highest compared with lowest d-dimer category had a 3.11-fold higher odds of death (95% CI, 2.56-3.77) in univariate analyses, decreasing to a 1.81-fold increased odds of death (95% CI, 1.43-2.28) after multivariable adjustment for demographics, comorbidities, and illness severity. Further adjustment for therapeutic anticoagulation did not meaningfully attenuate this relationship (odds ratio, 1.73; 95% CI, 1.36-2.19).
Conclusions: In a large multicenter cohort study of critically ill patients with coronavirus disease 2019, higher d-dimer levels were independently associated with a greater risk of death.
Trial registration: ClinicalTrials.gov NCT04401293.
Copyright © 2021 by the Society of Critical Care Medicine and Wolters Kluwer Health, Inc. All Rights Reserved.
Conflict of interest statement
Dr. Gupta’s institution received funding from the Foundation for the National Institutes of Health (NIH) 5 F32 DC 17342-2; she received funding from GlaxoSmithKline; she is a scientific coordinator for the Anemia Studies in CKD: Erythropoiesis via a Novel Prolyl Hydroxylase Inhibitor Daprodustat (ASCEND) trial (GlaskoSmithKline). Dr. Srivastava received funding from CVS Caremark, AstraZeneca, Horizon Therapeutics, PLC, and Tate & Latham. Dr. Shaefi’s institution received funding from the National Institute on Aging/NIH R03AG060179 and the National Institute of General Medical Sciences/NIH K08GM134220; he received support for article research from the NIH. Dr. Bagchi's institution received funding from the American Heart Association 20IPA35360009. He received funding from Lungpacer Medical, Inc. Dr. Al-Samkari received funding from Agios, Dova, Rigel, Argenx, and Amgen. Dr. Zakai’s institution received funding from the NIH and Centers for Disease Control and Prevention. Dr. Leaf received research support from BioPorto. The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
References
-
- Home: Johns Hopkins Coronavirus Resource Center. Available at: https://coronavirus.jhu.edu/. Accessed October 15, 2020
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
