

Associations of Maternal Cardiovascular Health in Pregnancy With Offspring Cardiovascular Health in Early Adolescence
- PMID: 33591345
- PMCID: PMC7887661
- DOI: 10.1001/jama.2021.0247
Associations of Maternal Cardiovascular Health in Pregnancy With Offspring Cardiovascular Health in Early Adolescence
Abstract
Importance: Pregnancy may be a key window to optimize cardiovascular health (CVH) for the mother and influence lifelong CVH for her child.
Objective: To examine associations between maternal gestational CVH and offspring CVH.
Design, setting, and participants: This cohort study used data from the Hyperglycemia and Adverse Pregnancy Outcome (HAPO) Study (examinations: July 2000-April 2006) and HAPO Follow-Up Study (examinations: February 2013-December 2016). The analyses included 2302 mother-child dyads, comprising 48% of HAPO Follow-Up Study participants, in an ancillary CVH study. Participants were from 9 field centers across the United States, Barbados, United Kingdom, China, Thailand, and Canada.
Exposures: Maternal gestational CVH at a target of 28 weeks' gestation, based on 5 metrics: body mass index, blood pressure, total cholesterol level, glucose level, and smoking. Each metric was categorized as ideal, intermediate, or poor using pregnancy guidelines. Total CVH was categorized as follows: all ideal metrics, 1 or more intermediate (but 0 poor) metrics, 1 poor metric, or 2 or more poor metrics.
Main outcomes and measures: Offspring CVH at ages 10 to 14 years, based on 4 metrics: body mass index, blood pressure, total cholesterol level, and glucose level. Total CVH was categorized as for mothers.
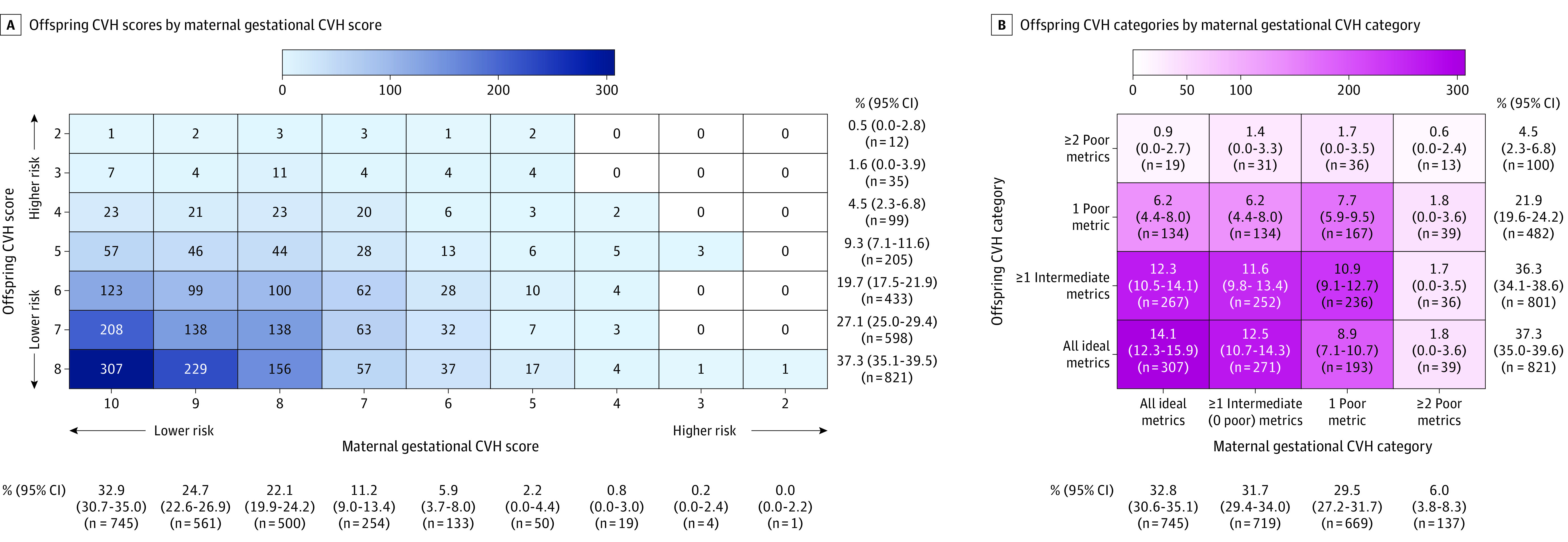
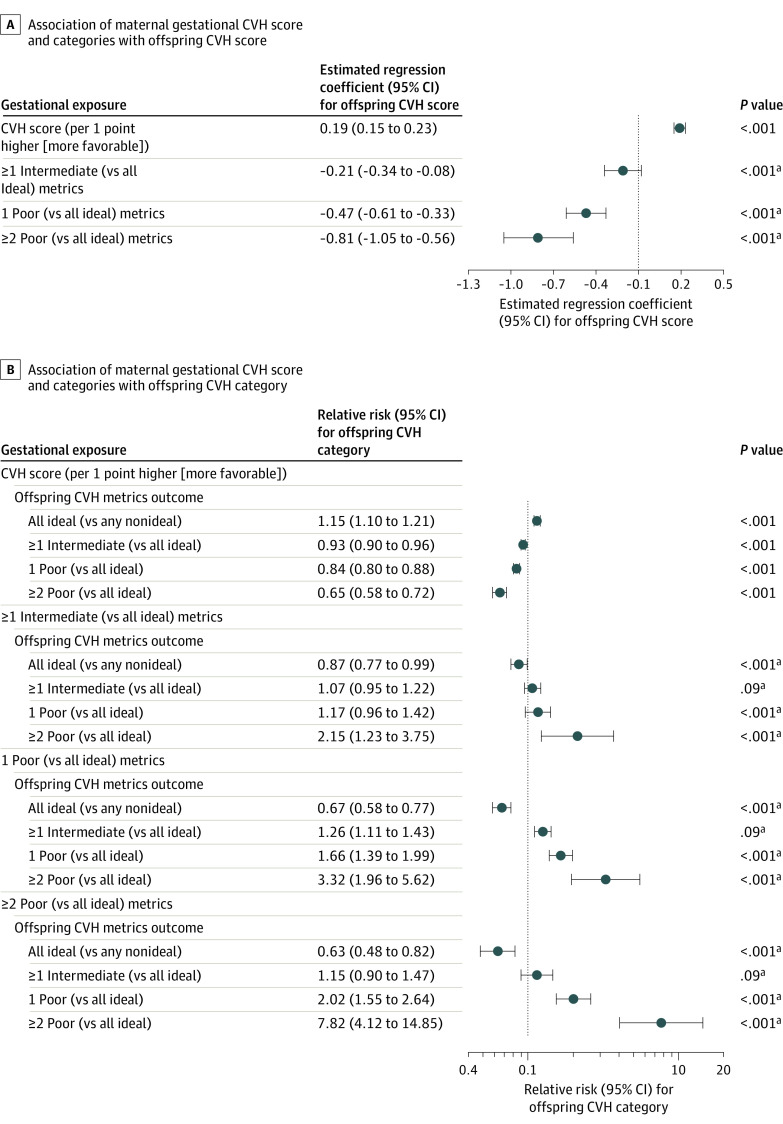
Results: Among 2302 dyads, the mean (SD) ages were 29.6 (2.7) years for pregnant mothers and 11.3 (1.1) years for children. During pregnancy, the mean (SD) maternal CVH score was 8.6 (1.4) out of 10. Among pregnant mothers, the prevalence of all ideal metrics was 32.8% (95% CI, 30.6%-35.1%), 31.7% (95% CI, 29.4%-34.0%) for 1 or more intermediate metrics, 29.5% (95% CI, 27.2%-31.7%) for 1 poor metric, and 6.0% (95% CI, 3.8%-8.3%) for 2 or more poor metrics. Among children of mothers with all ideal metrics, the prevalence of all ideal metrics was 42.2% (95% CI, 38.4%-46.2%), 36.7% (95% CI, 32.9%-40.7%) for 1 or more intermediate metrics, 18.4% (95% CI, 14.6%-22.4%) for 1 poor metric, and 2.6% (95% CI, 0%-6.6%) for 2 or more poor metrics. Among children of mothers with 2 or more poor metrics, the prevalence of all ideal metrics was 30.7% (95% CI, 22.0%-40.4%), 28.3% (95% CI, 19.7%-38.1%) for 1 or more intermediate metrics, 30.7% (95% CI, 22.0%-40.4%) for 1 poor metric, and 10.2% (95% CI, 1.6%-20.0%) for 2 or more poor metrics. The adjusted relative risks associated with 1 or more intermediate, 1 poor, and 2 or more poor (vs all ideal) metrics, respectively, in mothers during pregnancy were 1.17 (95% CI, 0.96-1.42), 1.66 (95% CI, 1.39-1.99), and 2.02 (95% CI, 1.55-2.64) for offspring to have 1 poor (vs all ideal) metrics, and the relative risks were 2.15 (95% CI, 1.23-3.75), 3.32 (95% CI,1.96-5.62), and 7.82 (95% CI, 4.12-14.85) for offspring to have 2 or more poor (vs all ideal) metrics. Additional adjustment for categorical birth factors (eg, preeclampsia) did not fully explain these significant associations (eg, relative risk for association between 2 or more poor metrics among mothers during pregnancy and 2 or more poor metrics among offspring after adjustment for an extended set of birth factors, 6.23 [95% CI, 3.03-12.82]).
Conclusions and relevance: In this multinational cohort, better maternal CVH at 28 weeks' gestation was significantly associated with better offspring CVH at ages 10 to 14 years.
Conflict of interest statement
Figures
Comment in
-
Maternal Cardiovascular Health: A Critical Period for Offspring Lifetime Cardiovascular Health?JAMA. 2021 Feb 16;325(7):630-631. doi: 10.1001/jama.2021.0134. JAMA. 2021. PMID: 33591330 No abstract available.
-
Prednison wirksam bei Gabe zu Beginn einer Clusterattacke.MMW Fortschr Med. 2021 Apr;163(6):28. doi: 10.1007/s15006-021-9772-3. MMW Fortschr Med. 2021. PMID: 33783782 German. No abstract available.
-
Wenn Mama kardiovaskulär gesund ist, sind es die Kinder später auch.MMW Fortschr Med. 2021 Apr;163(6):28-30. doi: 10.1007/s15006-021-9771-4. MMW Fortschr Med. 2021. PMID: 33783783 German. No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
