

Effect of High-Intensity Strength Training on Knee Pain and Knee Joint Compressive Forces Among Adults With Knee Osteoarthritis: The START Randomized Clinical Trial
- PMID: 33591346
- PMCID: PMC7887656
- DOI: 10.1001/jama.2021.0411
Effect of High-Intensity Strength Training on Knee Pain and Knee Joint Compressive Forces Among Adults With Knee Osteoarthritis: The START Randomized Clinical Trial
Abstract
Importance: Thigh muscle weakness is associated with knee discomfort and osteoarthritis disease progression. Little is known about the efficacy of high-intensity strength training in patients with knee osteoarthritis or whether it may worsen knee symptoms.
Objective: To determine whether high-intensity strength training reduces knee pain and knee joint compressive forces more than low-intensity strength training and more than attention control in patients with knee osteoarthritis.
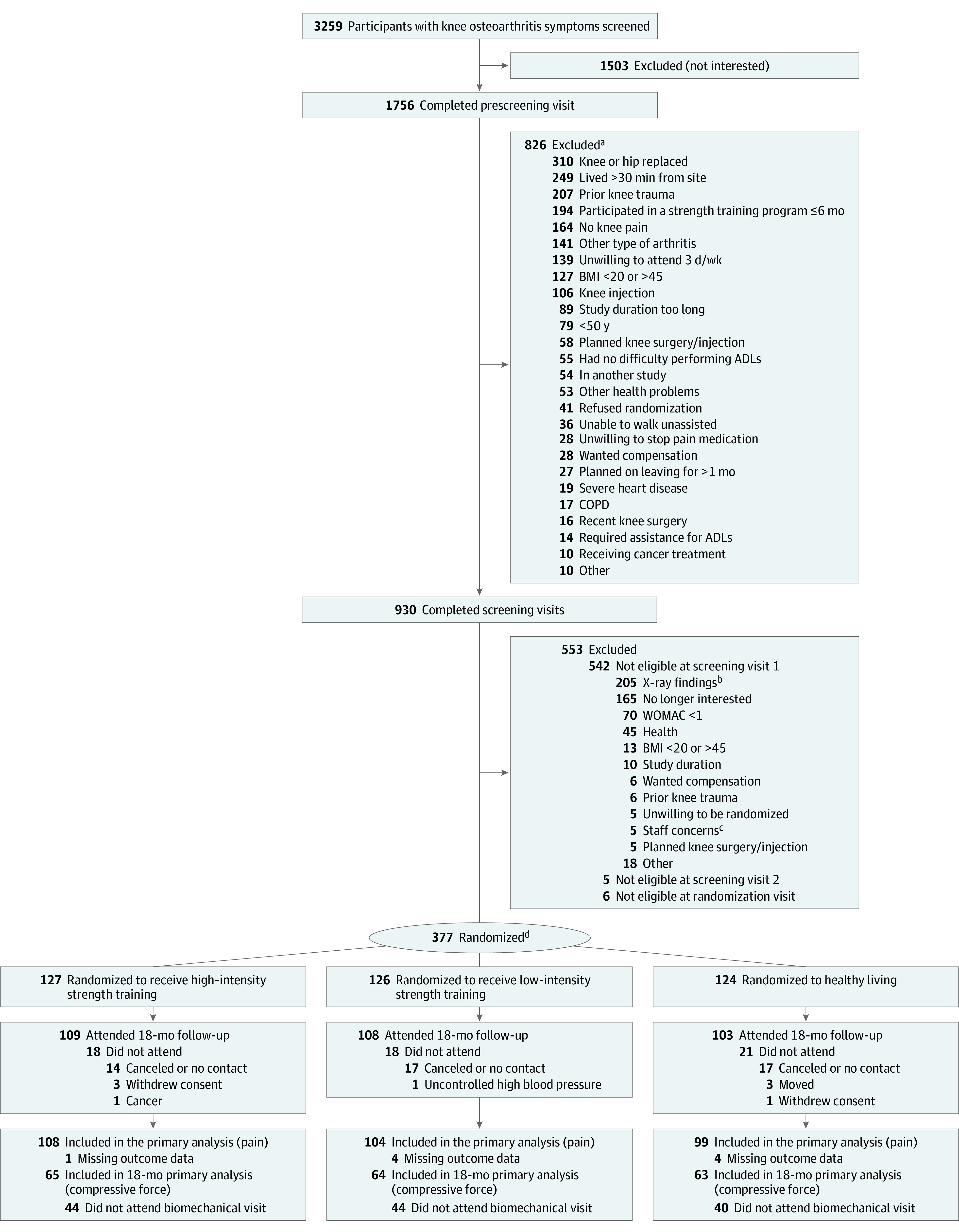
Design, setting, and participants: Assessor-blinded randomized clinical trial conducted at a university research center in North Carolina that included 377 community-dwelling adults (≥50 years) with body mass index (BMI) ranging from 20 to 45 and with knee pain and radiographic knee osteoarthritis. Enrollment occurred between July 2012 and February 2016, and follow-up was completed September 2017.
Interventions: Participants were randomized to high-intensity strength training (n = 127), low-intensity strength training (n = 126), or attention control (n = 124).
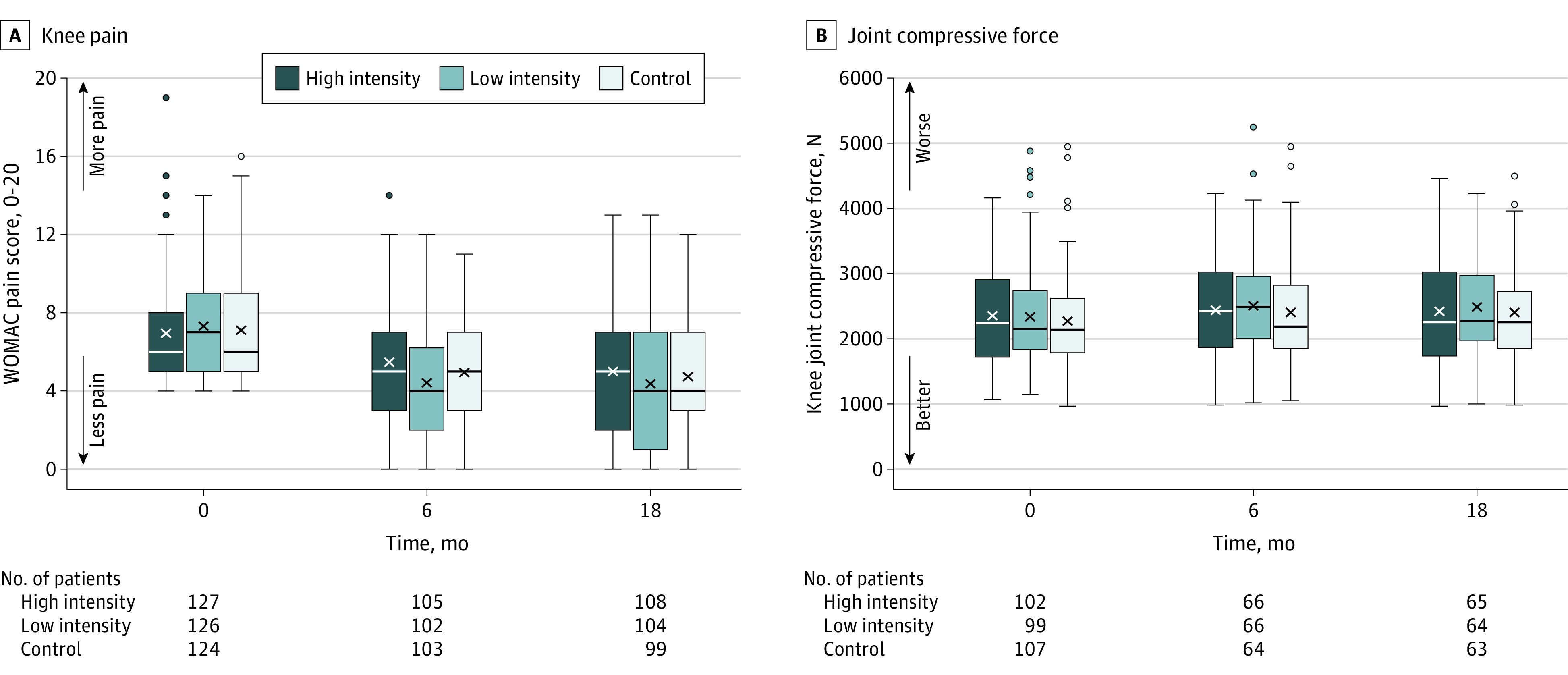
Main outcomes and measures: Primary outcomes at the 18-month follow-up were Western Ontario McMaster Universities Osteoarthritis Index (WOMAC) knee pain (0 best-20 worst; minimally clinically important difference [MCID, 2]) and knee joint compressive force, defined as the maximal tibiofemoral contact force exerted along the long axis of the tibia during walking (MCID, unknown).
Results: Among 377 randomized participants (mean age, 65 years; 151 women [40%]), 320 (85%) completed the trial. Mean adjusted (sex, baseline BMI, baseline outcome values) WOMAC pain scores at the 18-month follow-up were not statistically significantly different between the high-intensity group and the control group (5.1 vs 4.9; adjusted difference, 0.2; 95% CI, -0.6 to 1.1; P = .61) or between the high-intensity and low-intensity groups (5.1 vs 4.4; adjusted difference, 0.7; 95% CI, -0.1 to 1.6; P = .08). Mean knee joint compressive forces were not statistically significantly different between the high-intensity group and the control group (2453 N vs 2512 N; adjusted difference, -58; 95% CI, -282 to 165 N; P = .61), or between the high-intensity and low-intensity groups (2453 N vs 2475 N; adjusted difference, -21; 95% CI, -235 to 193 N; P = .85). There were 87 nonserious adverse events (high-intensity, 53; low-intensity, 30; control, 4) and 13 serious adverse events unrelated to the study (high-intensity, 5; low-intensity, 3; control, 5).
Conclusions and relevance: Among patients with knee osteoarthritis, high-intensity strength training compared with low-intensity strength training or an attention control did not significantly reduce knee pain or knee joint compressive forces at 18 months. The findings do not support the use of high-intensity strength training over low-intensity strength training or an attention control in adults with knee osteoarthritis.
Trial registration: ClinicalTrials.gov Identifier: NCT01489462.
Conflict of interest statement
Figures
Comment in
-
High-Intensity Strength Training, Knee Pain, and Knee Joint Compressive Forces in Adults With Knee Osteoarthritis.JAMA. 2021 Jun 8;325(22):2315-2316. doi: 10.1001/jama.2021.6000. JAMA. 2021. PMID: 34100874 No abstract available.
References
-
- Hall M, Hinman RS, Wrigley TV, Kasza J, Lim B-W, Bennell KL. Knee extensor strength gains mediate symptom improvement in knee osteoarthritis: secondary analysis of a randomised controlled trial. Osteoarthritis Cartilage. 2018;26(4):495-500. - PubMed
-
- Singh NA, Clements KM, Fiatarone MA. A randomized controlled trial of progressive resistance training in depressed elders. J Gerontol A Biol Sci Med Sci. 1997;52(1):M27-M35. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
