

Trends in Low-Value Health Service Use and Spending in the US Medicare Fee-for-Service Program, 2014-2018
- PMID: 33591365
- PMCID: PMC7887655
- DOI: 10.1001/jamanetworkopen.2020.37328
Trends in Low-Value Health Service Use and Spending in the US Medicare Fee-for-Service Program, 2014-2018
Abstract
Importance: Low-value care, defined as care offering no net benefit in specific clinical scenarios, is associated with harmful outcomes in patients and wasteful spending. Despite a national education campaign and increasing attention on reducing health care waste, recent trends in low-value care delivery remain unknown.
Objective: To assess national trends in low-value care use and spending.
Design, setting, and participants: In this cross-sectional study, analyses of low-value care use and spending from 2014 to 2018 were conducted using 100% Medicare fee-for-service enrollment and claims data. Included individuals were aged 65 years or older and continuously enrolled in Medicare parts A, B, and D during each measurement year and the previous year. Data were analyzed from September 2019 through December 2020.
Exposure: Being enrolled in fee-for-service Medicare for a period of time, in years.
Main outcomes and measures: The Milliman MedInsight Health Waste Calculator was used to assess 32 claims-based measures of low-value care associated with Choosing Wisely recommendations and other professional guidelines. The calculator designates services as wasteful, likely wasteful, or not wasteful based on an absence of indication of appropriate use in the claims history; calculator-designated wasteful services were defined as low-value care. Spending was calculated as claim-line level (ie, spending on the low-value service) and claim level (ie, spending on the low-value service plus associated services), adjusting for inflation.
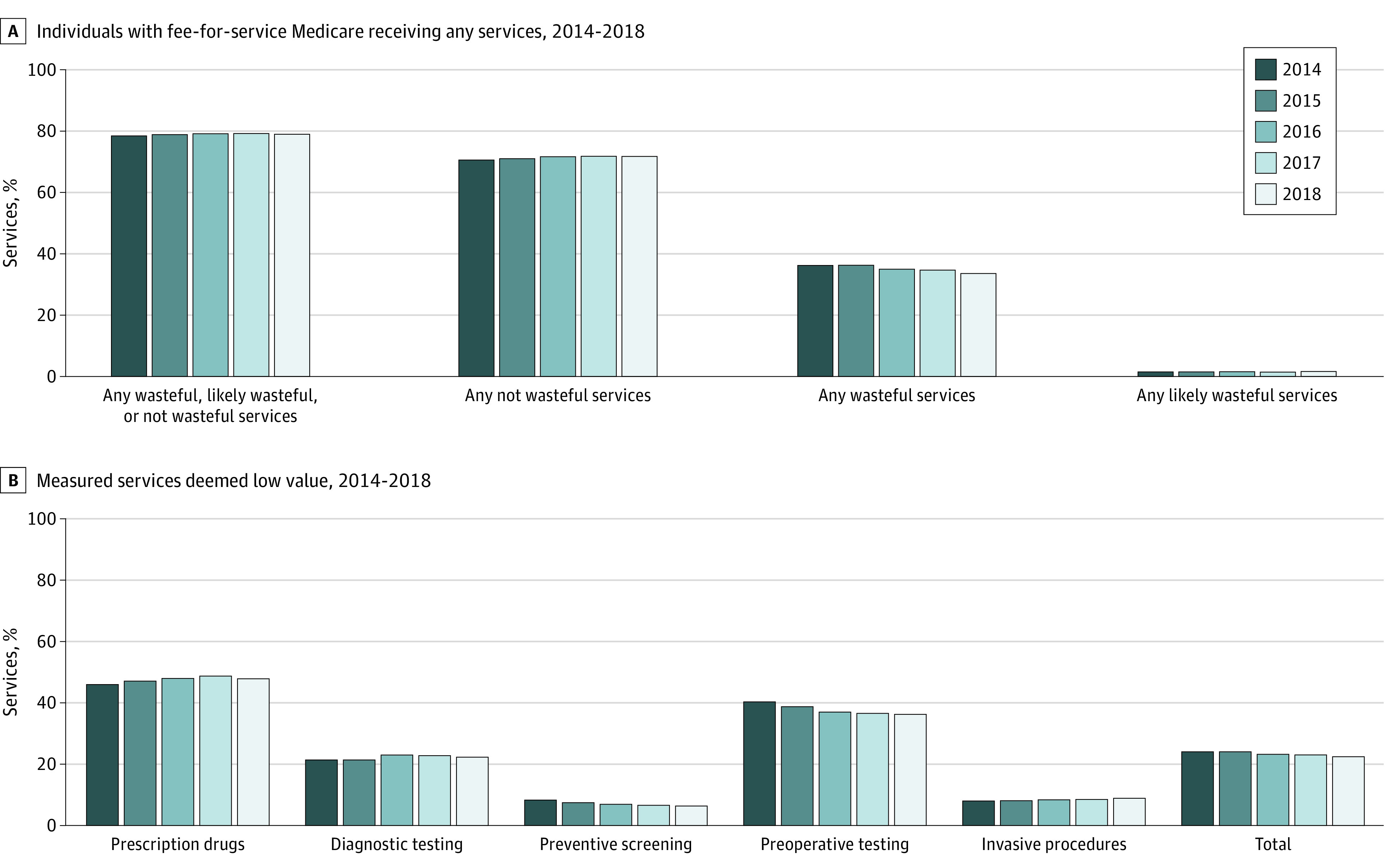
Results: Among 21 045 759 individuals with fee-for-service Medicare (mean [SD] age, 77.4 [7.9] years; 12 515 915 [59.5%] women), the percentage receiving any of 32 low-value services decreased from 36.3% (95% CI, 36.3%-36.4%) to 33.6% (95% CI, 33.6%-33.6%) from 2014 to 2018. Uses of low-value services per 1000 individuals decreased from 677.8 (95% CI, 676.2-679.5) to 632.7 (95% CI, 632.6-632.8) from 2014 to 2018. Three services comprised approximately two-thirds of uses among 32 low-value services per 1000 individuals: preoperative laboratory testing decreased from 213.8 (95% CI, 213.4-214.2) to 166.2 (95% CI, 166.2-166.2), while opioids for back pain increased from 154.4 (95% CI, 153.6-155.2) to 182.1 (95% CI, 182.1-182.1) and antibiotics for upper respiratory infections increased from 75.0 (95% CI, 75.0-75.1) to 82 (95% CI, 82.0-82.0). Spending per 1000 individuals on low-value care also decreased, from $52 765.5 (95% CI, $51 952.3-$53 578.6) to $46 921.7 (95% CI, $46 593.7-$47 249.7) at the claim-line level and from $160 070.4 (95% CI, $158 999.8-$161 141.0) to $144 741.1 (95% CI, $144 287.5-$145 194.7) at the claim level.
Conclusions and relevance: This cross-sectional study found that among individuals with fee-for-service Medicare receiving any of 32 measured services, low-value care use and spending decreased marginally from 2014 to 2018, despite a national education campaign in collaboration with clinician specialty societies and increased attention on low-value care. While most use of low-value care came from 3 services, 1 of these was opioid prescriptions, which increased over time despite the harms associated with their use. These findings may represent several opportunities to prevent patient harm and lower spending.
Conflict of interest statement
Figures
References
-
- Institute of Medicine Best Care at Lower Cost: The Path to Continuously Learning Health Care in America. The National Academies Press; 2013. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
