

Haloperidol, clonidine and resolution of delirium in critically ill patients: a prospective cohort study
- PMID: 33591422
- PMCID: PMC7952362
- DOI: 10.1007/s00134-021-06355-9
Haloperidol, clonidine and resolution of delirium in critically ill patients: a prospective cohort study
Abstract
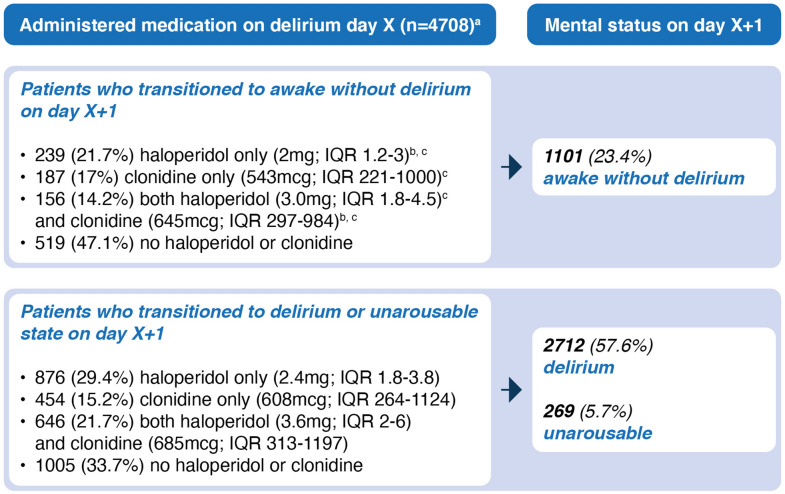
Purpose: Haloperidol and clonidine are commonly used to treat agitation in delirious intensive care unit (ICU) patients, but it is unclear whether these agents may shorten the duration of delirium. The objective of this study was to determine whether haloperidol, clonidine, or their combined administration to delirious ICU patients results in delirium resolution.
Methods: This was a cohort study on a mixed ICU, excluding patients with a primary neurological disorder. The main outcome was the probability of delirium resolution, using propensity score matching and Markov multinomial logistic regression models for daily transitions. Secondary outcomes were delirium duration, number of delirium days, ventilation days, length of stay in the ICU and hospital, and ICU mortality.
Results: A total of 3614 patients were included (1165 delirious [32%]; 2449 non-delirious [68%]). Delirium occurred on 4708 (18.9%) of 24,906 days. The probability of delirium resolution was lower in delirious patients who received haloperidol (OR 0.47, 95% CI 0.39-0.57), clonidine (OR 0.78, 95% CI 0.63-0.97), or both (OR 0.45, 95% CI 0.36-0.56) compared to untreated delirious patients. Delirious patients who received haloperidol, clonidine, or both had generally longer delirium duration, more delirium and ventilation days, and spent more time in the ICU and in hospital than untreated delirious patients. These agents had no effect on ICU mortality.
Conclusion: Haloperidol and clonidine use in delirious ICU patients may be associated with reduced probability of delirium resolution. This finding, however, merits further investigation given inherent limitations of this observational analysis.
Keywords: Clonidine; Critical care; Delirium; Haloperidol; Intensive care unit.
Conflict of interest statement
All authors declare no conflicts of interest.
Figures
Comment in
-
[Focus on neurological intensive care medicine. Intensive care studies from 2020/2021].Anaesthesist. 2021 Aug;70(8):706-713. doi: 10.1007/s00101-021-00977-w. Epub 2021 Jun 30. Anaesthesist. 2021. PMID: 34191035 Free PMC article. German. No abstract available.
References
-
- Ely EW, Girard TD, Shintani AK, Jackson JC, et al. Apolipoprotein E4 polymorphism as a genetic predisposition to delirium in critically ill patients. Crit Care Med. 2007;35(1):112–117. doi: 10.1097/01.CCM.0000251925.18961.CA. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
