

An autophagic gene-based signature to predict the survival of patients with low-grade gliomas
- PMID: 33591634
- PMCID: PMC7940225
- DOI: 10.1002/cam4.3748
An autophagic gene-based signature to predict the survival of patients with low-grade gliomas
Abstract
Background: Since autophagy remains an important topic of investigation, the RNA-sequence profiles of autophagy-related genes (ARGs) can provide insights into predicting low-grade gliomas (LGG) prognosis.
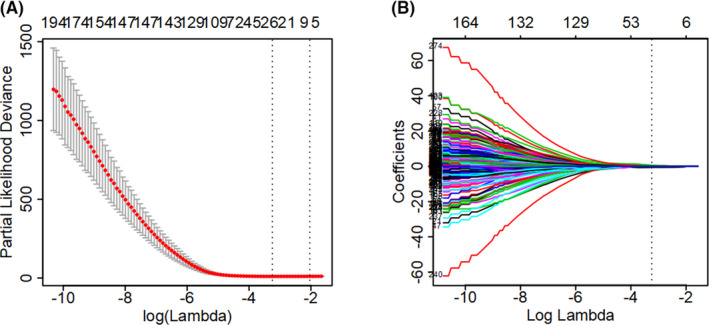
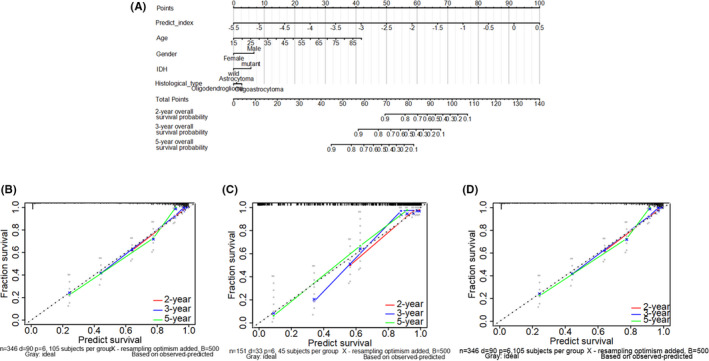
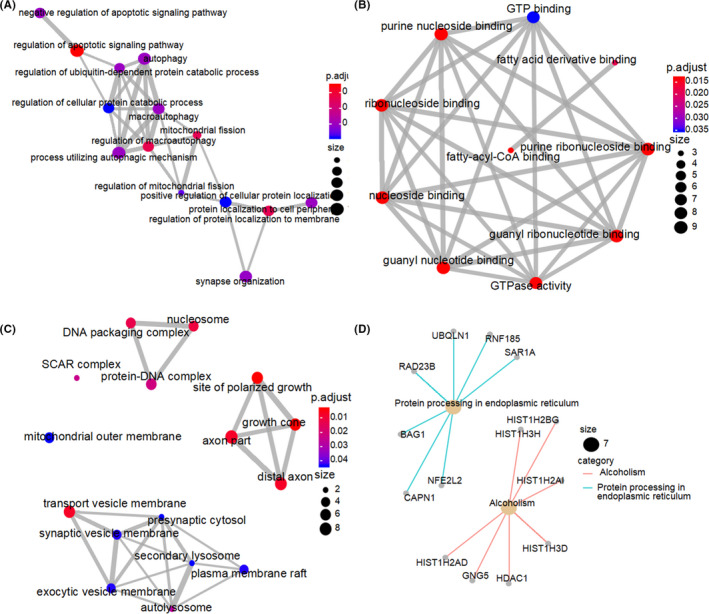
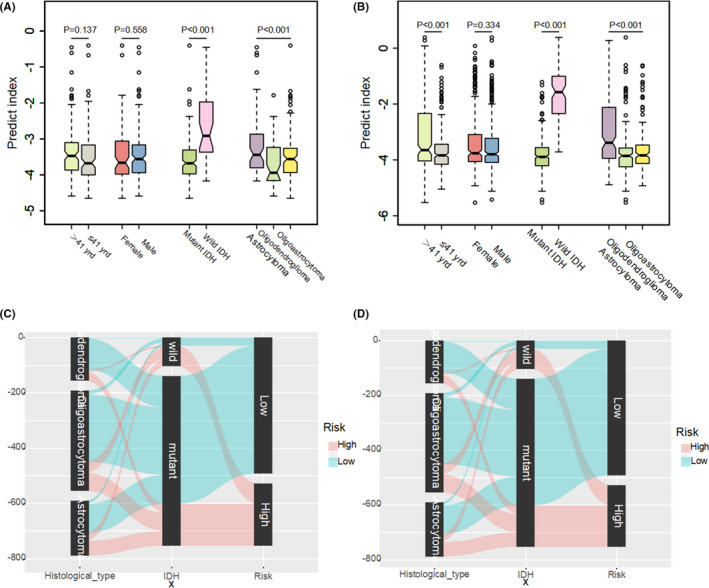
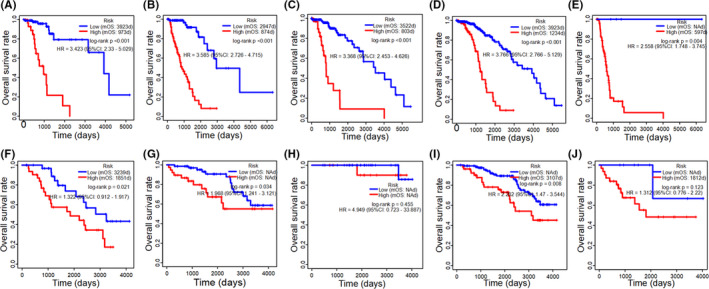
Methods: The RNA-seq profiles of autophagic genes and prognosis data of LGG were integrated from the Cancer Genome Atlas (TCGA) and Chinese Glioma Genome Atlas (CGGA). Univariate Cox analysis and the least absolute shrinkage and selection operator (LASSO) regression model were carried out to identify the differentially expressed prognostic autophagy-related genes. Then, the autophagic-gene signature was formed and verified in TCGA test set and external CGGA cohorts. Time-dependent receiver operating characteristic (ROC) was examined to test the accuracy of this signature feature. A nomogram was conducted to meet the needs of clinicians. Sankey diagrams were performed to visualize the relationship between the multigene signatures and clinic-pathological features.
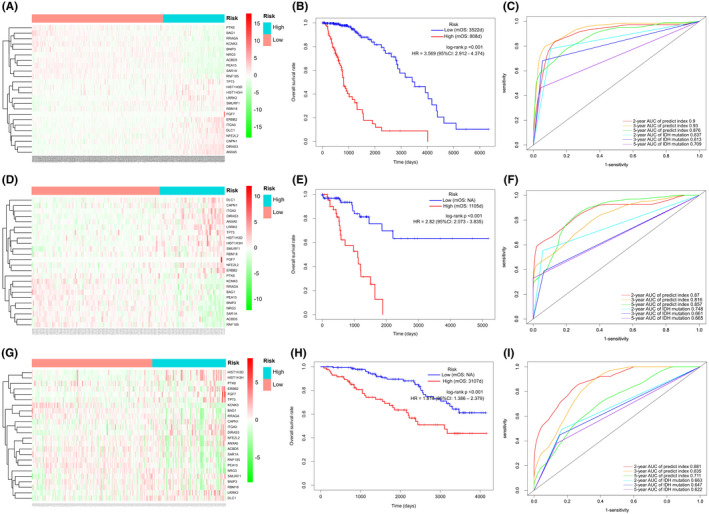
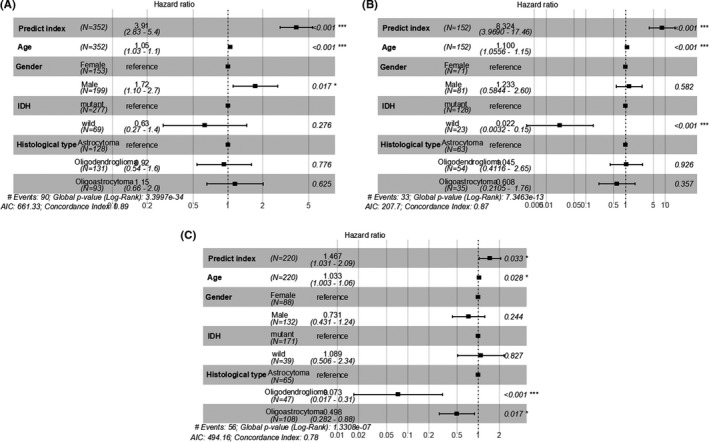
Results: Twenty-four ARGs were finally identified most relevant to LGG prognosis. According to the specific prediction index formula, the patients were classified into low-risk or high-risk groups. Prognostic accuracy was proved by time-dependent ROC analysis, with AUC 0.9, 0.93, and 0.876 at the survival time of 2-, 3-, and 5-year, respectively, which was superior to the AUC of the isocitrate dehydrogenase (IDH) mutation. The result was confirmed while validated in the TCGA test set and external validation CGGA cohort. A nomogram was constructed to meet individual needs. With a visualization approach, Sankey diagrams show the relationship of the histological type, IDH status, and predict index. In TCGA and CGGA cohorts, both low-risk groups displayed better survival rate in LGG while histological type and IDH status did not show consistency results.
Conclusions: 24-ARGs may play crucial roles in the progression of LGG, and LGG patients were effectively divided into low-risk and high-risk groups according to prognostic prediction. Overall, our study will provide novel strategies for clinical applications.
Keywords: autophagy; low-grade gliomas; nomogram; prognosis.
© 2021 The Authors. Cancer Medicine published by John Wiley & Sons Ltd.
Conflict of interest statement
The authors declare that the research was conducted without any potential conflict of interest.
Figures
References
-
- Darlix A, Goze C, Rigau V, Bauchet L, Taillandier L, Duffau H. The etiopathogenesis of diffuse low‐grade gliomas. Crit Rev Oncol Hematol. 2017;109:51–62. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
