

Arrhythmias in Cardiac Sarcoidosis Bench to Bedside: A Case-Based Review
- PMID: 33591816
- PMCID: PMC8142901
- DOI: 10.1161/CIRCEP.120.009203
Arrhythmias in Cardiac Sarcoidosis Bench to Bedside: A Case-Based Review
Abstract
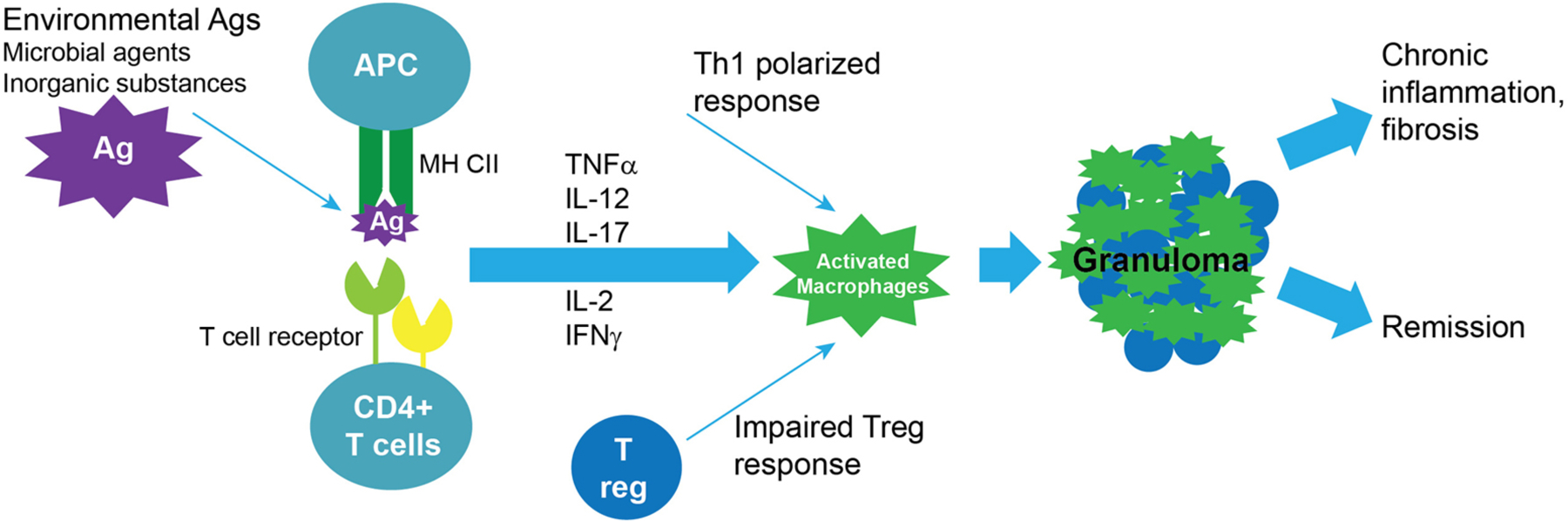
Cardiac sarcoidosis is a component of an often multiorgan granulomatous disease of still uncertain cause. It is being recognized with increasing frequency, mainly as the result of heightened awareness and new diagnostic tests, specifically cardiac magnetic resonance imaging and 18F-fluorodeoxyglucose positron emission tomography scans. The purpose of this case-based review is to highlight the potentially life-saving importance of making the early diagnosis of cardiac sarcoidosis using these new tools and to provide a framework for the optimal care of patients with this disease. We will review disease mechanisms as currently understood, associated arrhythmias including conduction abnormalities, and atrial and ventricular tachyarrhythmias, guideline-directed diagnostic criteria, screening of patients with extracardiac sarcoidosis, and the use of pacemakers and defibrillators in this setting. Treatment options, including those related to heart failure, and those which may help clarify disease mechanisms are included.
Keywords: atrial fibrillation; bradycardia; defibrillator; heart failure; sarcoidosis; tachycardia.
Figures
Similar articles
-
Outcome of catheter ablation of supraventricular tachyarrhythmias in cardiac sarcoidosis.Clin Cardiol. 2019 Nov;42(11):1121-1125. doi: 10.1002/clc.23263. Epub 2019 Sep 3. Clin Cardiol. 2019. PMID: 31482624 Free PMC article.
-
Atrial Arrhythmias in Clinically Manifest Cardiac Sarcoidosis: Incidence, Burden, Predictors, and Outcomes.J Am Heart Assoc. 2020 Sep;9(17):e017086. doi: 10.1161/JAHA.120.017086. Epub 2020 Aug 20. J Am Heart Assoc. 2020. PMID: 32814465 Free PMC article. Clinical Trial.
-
Evaluation and management of heart rhythm disturbances due to cardiac sarcoidosis.Heart Lung Circ. 2014 Dec;23(12):1100-9. doi: 10.1016/j.hlc.2014.07.065. Epub 2014 Jul 29. Heart Lung Circ. 2014. PMID: 25130888 Review.
-
Response to steroid therapy in cardiac sarcoidosis: insights from myocardial strain.Eur Heart J Cardiovasc Imaging. 2012 Feb;13(2):E3. doi: 10.1093/ejechocard/jer184. Epub 2011 Oct 11. Eur Heart J Cardiovasc Imaging. 2012. PMID: 21990278
-
[Cardiac sarcoidosis: diagnostics, treatment and follow-up].Pol Merkur Lekarski. 2018 Mar 27;44(261):124-129. Pol Merkur Lekarski. 2018. PMID: 29601561 Review. Polish.
Cited by
-
Evaluation and Catheter Ablation of Ventricular Arrhythmias in Cardiac Sarcoidosis.J Clin Med. 2022 Nov 13;11(22):6718. doi: 10.3390/jcm11226718. J Clin Med. 2022. PMID: 36431195 Free PMC article. Review.
-
Preventing Deadly Complications of Cardiac Sarcoidosis.Cureus. 2023 Jun 30;15(6):e41175. doi: 10.7759/cureus.41175. eCollection 2023 Jun. Cureus. 2023. PMID: 37525790 Free PMC article.
-
Arrhythmia Monitoring and Outcomes in Patients With Cardiac Sarcoidosis: Insights From the Cardiac Sarcoidosis Consortium.J Am Heart Assoc. 2022 Jul 5;11(13):e024924. doi: 10.1161/JAHA.121.024924. Epub 2022 Jun 22. J Am Heart Assoc. 2022. PMID: 35730638 Free PMC article. No abstract available.
-
Surprising palpitation: An unexpected diagnosis of sarcoidosis.ARYA Atheroscler. 2025;21(2):3-9. doi: 10.48305/arya.2024.42684.2968. ARYA Atheroscler. 2025. PMID: 40463845 Free PMC article.
-
Incidence of Sudden Cardiac Death and Life-Threatening Arrhythmias in Clinically Manifest Cardiac Sarcoidosis With and Without Current Indications for an Implantable Cardioverter Defibrillator.Circulation. 2022 Sep 27;146(13):964-975. doi: 10.1161/CIRCULATIONAHA.121.058120. Epub 2022 Aug 24. Circulation. 2022. PMID: 36000392 Free PMC article.
References
-
- Nordenswan HK, Lehtonen J, Ekstrom K, Kandolin R, Simonen P, Mayranpaa M, Vihinen T, Miettinen H, Kaikkonen K, Haataja P, et al. Outcome of Cardiac Sarcoidosis Presenting With High-Grade Atrioventricular Block. Circ Arrhythm Electrophysiol. 2018;11:e006145. - PubMed
-
- Diagnostic standard and guidelines for sarcoidosis. Japanese Journal of Sarcoidosis Granulomatous Disorders. 2007;27:89–102.
-
- Birnie DH, Sauer WH, Bogun F, Cooper JM, Culver DA, Duvernoy CS, Judson MA, Kron J, Mehta D, Nielsen JC, et al. HRS Expert Consensus Statement on the Diagnosis and Management of Arrhythmias Associated With Cardiac Sarcoidosis. Heart Rhythm. 2014;11:1304–1323. - PubMed
-
- Yoshinaga K, Miyagawa M, Kiso K, Ishida Y. Japanese Guidelines for Cardiac Sarcoidosis. Annals of Nuclear Cardiology. 2017;3:121–124.
-
- Terasaki F, Azuma A, Anzai T, Ishizaka N, Ishida Y, Isobe M, Inomata T, Ishibashi-Ueda H, Eishi Y, Kitakaze M, et al. JCS 2016 Guideline on Diagnosis and Treatment of Cardiac Sarcoidosis- Digest Version. Circ J. 2019;83:2329–2388. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
