

Contribution of Risk Factors to the Development of Coronary Atherosclerosis as Confirmed via Coronary CT Angiography: A Longitudinal Radiomics-based Study
- PMID: 33591887
- PMCID: PMC7997618
- DOI: 10.1148/radiol.2021203179
Contribution of Risk Factors to the Development of Coronary Atherosclerosis as Confirmed via Coronary CT Angiography: A Longitudinal Radiomics-based Study
Abstract
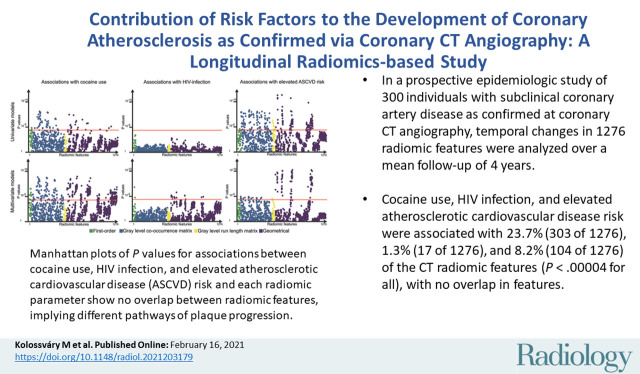
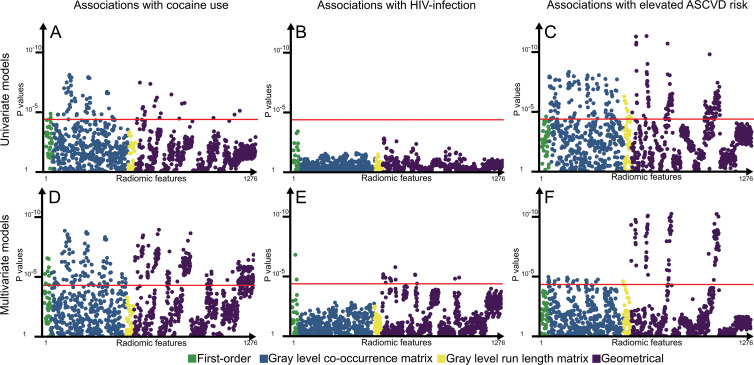
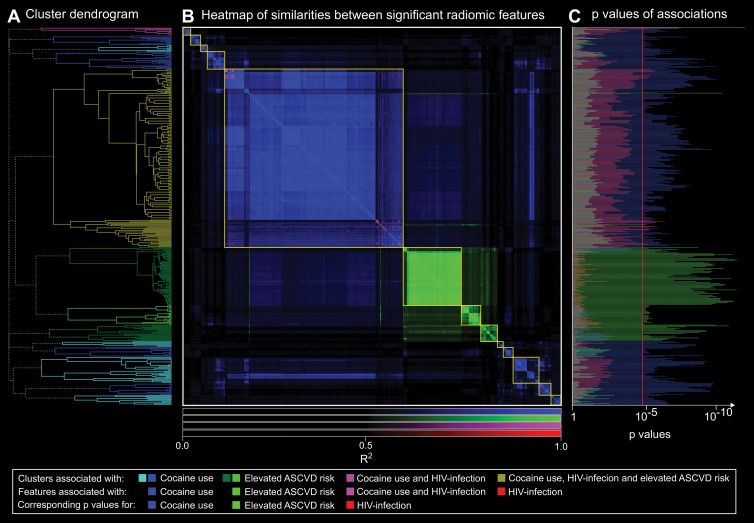
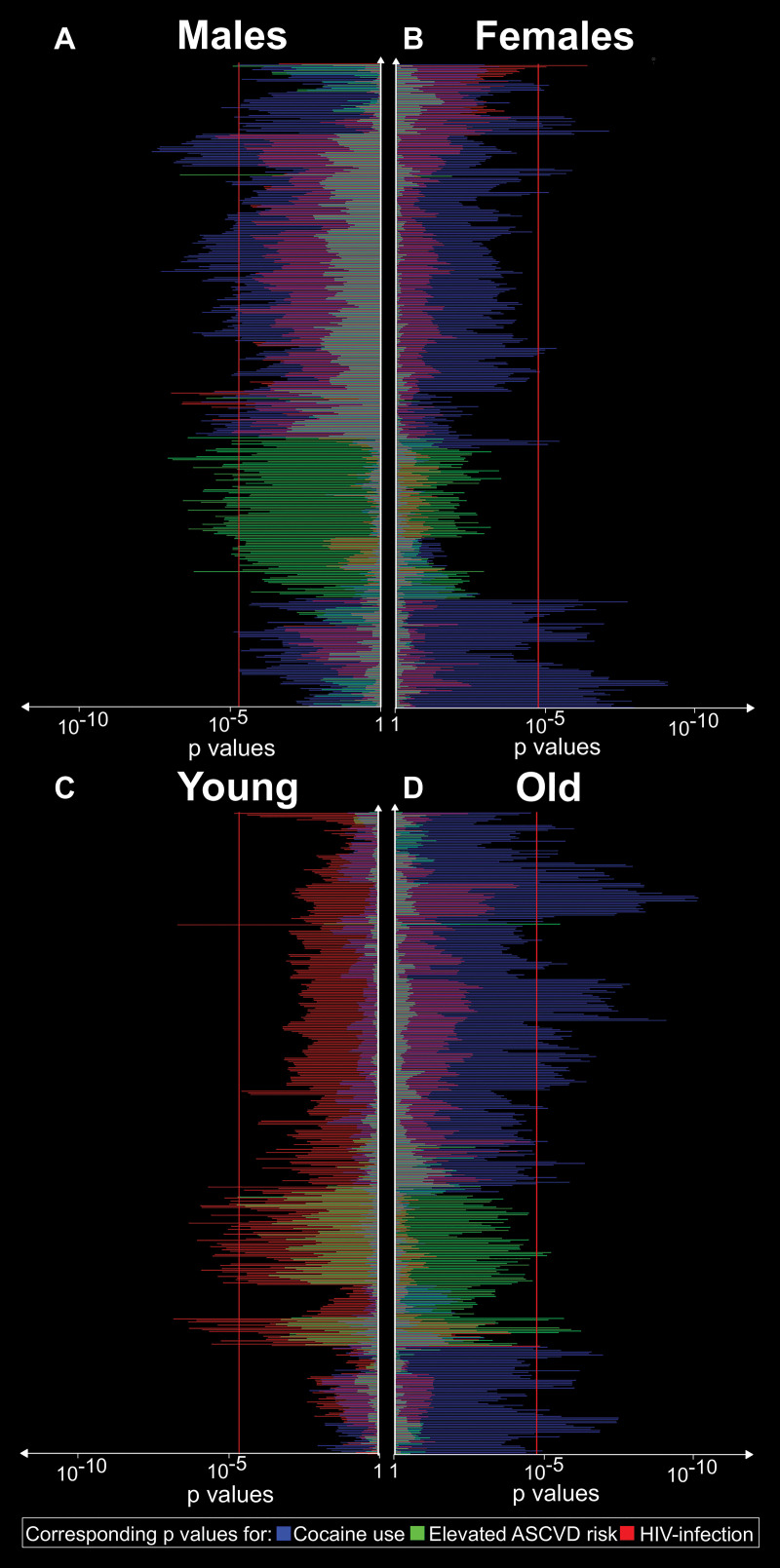
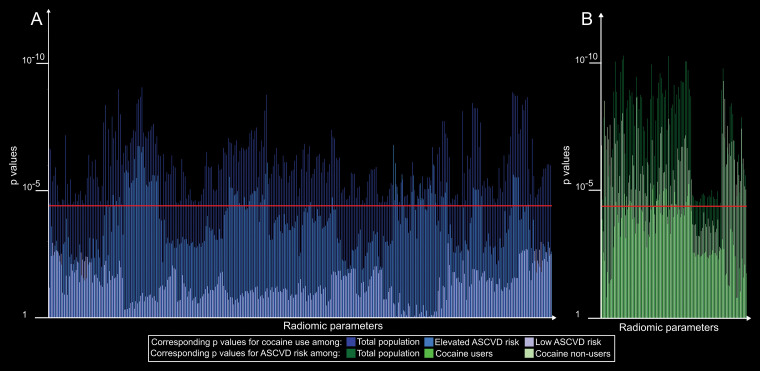
Background Various cardiovascular risk factors are thought to modify atherosclerosis in a similar fashion (ie, by increasing the magnitude of coronary artery disease [CAD]). However, coronary CT angiography allows precision phenotyping of plaque characteristics through use of radiomics. Purpose To assess whether different cardiovascular risk factors have distinctive contributions to the changes in plaque morphologic features over time. Materials and Methods Individuals with or without HIV infection and cocaine use and without cardiovascular symptoms underwent coronary CT angiography between May 2004 and August 2015. In the current HIPAA-compliant study, the effects of cocaine use, HIV infection, and atherosclerotic cardiovascular disease (ASCVD) risk on the temporal changes (mean ± standard deviation, 4.0 years ± 2.3 between CT angiographic examinations) in CAD structure were analyzed by using radiomic analysis. The changes in radiomic features were analyzed by using linear mixed models, with correction for factors that may change plaque structure: high-sensitivity C-reactive protein level, statin use, positive family history of CAD, and total plaque volume to account for any potential intrinsic correlation between volume and morphologic features. Clusters among significant radiomic features were identified by using hierarchical clustering. Bonferroni-corrected P values less than .00004 (.05 divided by 1276) were considered to indicate significant differences. Results Of 1429 participants, 300 with CAD confirmed at coronary CT angiography were randomly selected (mean age, 48 years ± 7; 210 men, 226 people infected with HIV, 174 people who use cocaine) and 1276 radiomic features were quantified for each plaque. Cocaine use was significantly associated with 23.7% (303 of 1276) of the radiomic features, HIV infection was significantly associated with 1.3% (17 of 1276), and elevated ASCVD risk was significantly associated with 8.2% (104 of 1276) (P < .00004 for all). Parameters associated with elevated ASCVD risk or cocaine use and HIV infection did not overlap. There were 13 clusters among the 409 parameters, eight of which were affected only by cocaine use and three of which were affected only by ASCVD risk. Conclusion Radiomics-based precision phenotyping indicated that conventional risk factors, cocaine use, and HIV infection each had different effects on CT angiographic morphologic changes in coronary atherosclerosis over 4 years. © RSNA, 2021 Online supplemental material is available for this article. See also the editorial by Schoepf and Emrich in this issue.
Figures
Comment in
-
A Brave New World: Toward Precision Phenotyping and Understanding of Coronary Artery Disease Using Radiomics Plaque Analysis.Radiology. 2021 Apr;299(1):107-108. doi: 10.1148/radiol.2021204456. Epub 2021 Feb 16. Radiology. 2021. PMID: 33595391 No abstract available.
Similar articles
-
Cardiovascular risk factors and illicit drug use may have a more profound effect on coronary atherosclerosis progression in people living with HIV.Eur Radiol. 2021 May;31(5):2756-2767. doi: 10.1007/s00330-021-07755-7. Epub 2021 Mar 3. Eur Radiol. 2021. PMID: 33660033 Free PMC article.
-
Temporal assessment of lesion morphology on radiological images beyond lesion volumes-a proof-of-principle study.Eur Radiol. 2022 Dec;32(12):8748-8760. doi: 10.1007/s00330-022-08894-1. Epub 2022 Jun 1. Eur Radiol. 2022. PMID: 35648210 Free PMC article.
-
Prevalence and Characterization of Subclinical Coronary Atherosclerotic Plaque with CT among Individuals with HIV: Results from the Canadian HIV and Aging Cohort Study.Radiology. 2021 Jun;299(3):571-580. doi: 10.1148/radiol.2021203297. Epub 2021 Apr 20. Radiology. 2021. PMID: 33876969
-
Impact of statin therapy on coronary plaque burden and composition assessed by coronary computed tomographic angiography: a systematic review and meta-analysis.Eur Heart J Cardiovasc Imaging. 2018 Aug 1;19(8):850-858. doi: 10.1093/ehjci/jey012. Eur Heart J Cardiovasc Imaging. 2018. PMID: 29617981
-
Non-invasive coronary imaging in elderly population.Eur J Radiol. 2023 May;162:110794. doi: 10.1016/j.ejrad.2023.110794. Epub 2023 Mar 22. Eur J Radiol. 2023. PMID: 37001255 Review.
Cited by
-
Deep Learning With Radiomics for Disease Diagnosis and Treatment: Challenges and Potential.Front Oncol. 2022 Feb 17;12:773840. doi: 10.3389/fonc.2022.773840. eCollection 2022. Front Oncol. 2022. PMID: 35251962 Free PMC article. Review.
-
Artificial intelligence in coronary computed tomography angiography: Demands and solutions from a clinical perspective.Front Cardiovasc Med. 2023 Feb 16;10:1120361. doi: 10.3389/fcvm.2023.1120361. eCollection 2023. Front Cardiovasc Med. 2023. PMID: 36873406 Free PMC article. Review.
-
Protocol and rationale of the Australian multicentre registry for serial cardiac computed tomography angiography (ARISTOCRAT): a prospective observational study of the natural history of pericoronary adipose tissue attenuation and radiomics.Cardiovasc Diagn Ther. 2024 Jun 30;14(3):447-458. doi: 10.21037/cdt-23-392. Epub 2024 Jun 27. Cardiovasc Diagn Ther. 2024. PMID: 38975008 Free PMC article.
-
Editorial: Radiomics in Cardiovascular Imaging.Front Cardiovasc Med. 2022 Apr 6;9:876713. doi: 10.3389/fcvm.2022.876713. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 35463760 Free PMC article. No abstract available.
-
Immune Dysregulation in Ischemic Heart Disease Among Individuals with Human Immunodeficiency Virus.Heart Fail Clin. 2025 Apr;21(2):227-239. doi: 10.1016/j.hfc.2024.12.005. Epub 2025 Jan 30. Heart Fail Clin. 2025. PMID: 40107801 Review.
References
-
- Arnett DK, Blumenthal RS, Albert MA, et al. . 2019 ACC/AHA guideline on the primary prevention of cardiovascular disease: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019;140(11):e563–e595. - PMC - PubMed
-
- Sytkowski PA, Kannel WB, D’Agostino RB. Changes in risk factors and the decline in mortality from cardiovascular disease. The Framingham Heart Study. N Engl J Med 1990;322(23):1635–1641. - PubMed
-
- Maurovich-Horvat P, Ferencik M, Voros S, Merkely B, Hoffmann U. Comprehensive plaque assessment by coronary CT angiography. Nat Rev Cardiol 2014;11(7):390–402. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
