

Accelerating elimination of sleeping sickness from the Guinean littoral through enhanced screening in the post-Ebola context: A retrospective analysis
- PMID: 33591980
- PMCID: PMC7909630
- DOI: 10.1371/journal.pntd.0009163
Accelerating elimination of sleeping sickness from the Guinean littoral through enhanced screening in the post-Ebola context: A retrospective analysis
Abstract
Background: Activities to control human African trypanosomiasis (HAT) in Guinea were severely hampered by the Ebola epidemic that hit this country between 2014 and 2016. Active screening was completely interrupted and passive screening could only be maintained in a few health facilities. At the end of the epidemic, medical interventions were progressively intensified to mitigate the risk of HAT resurgence and progress towards disease elimination.
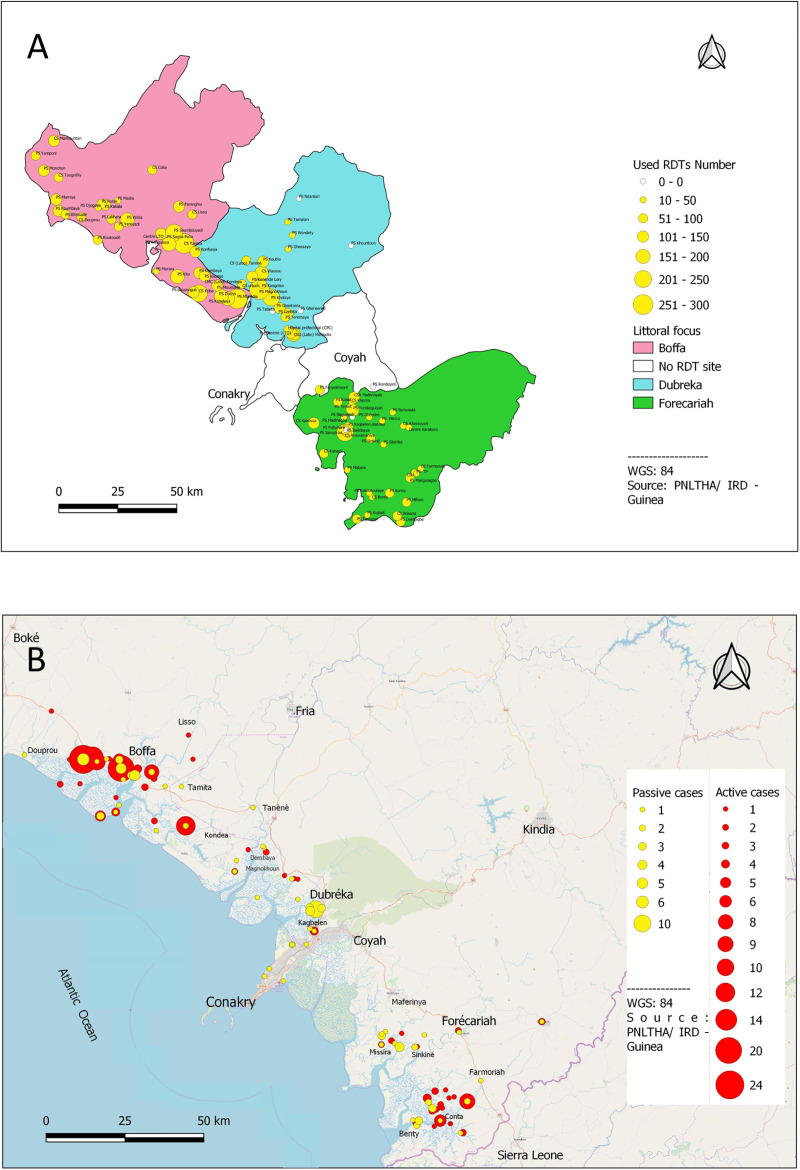
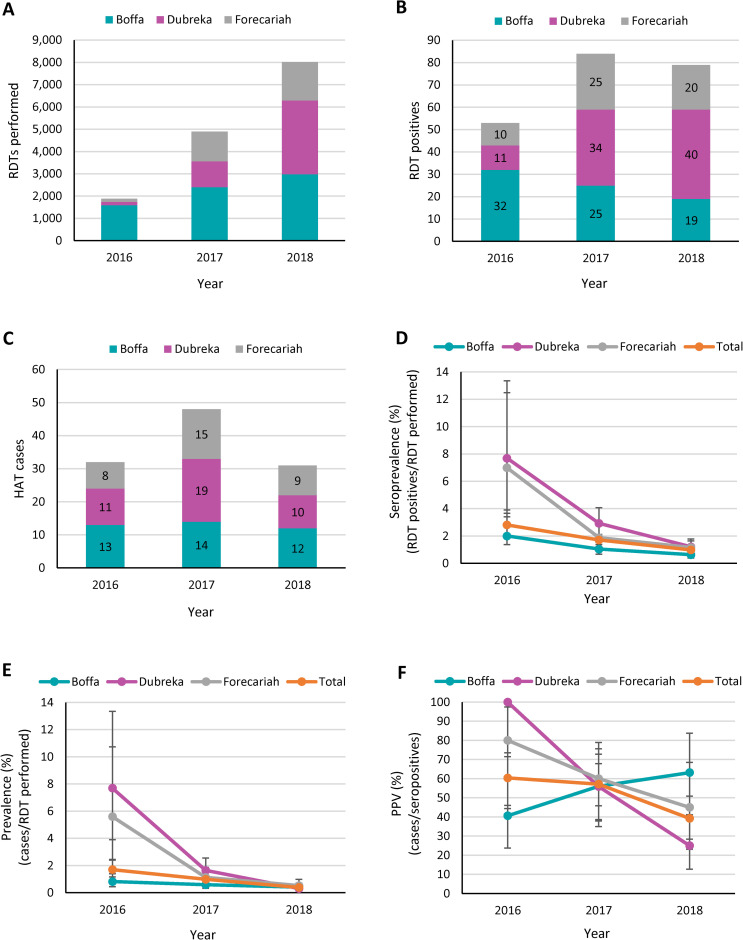
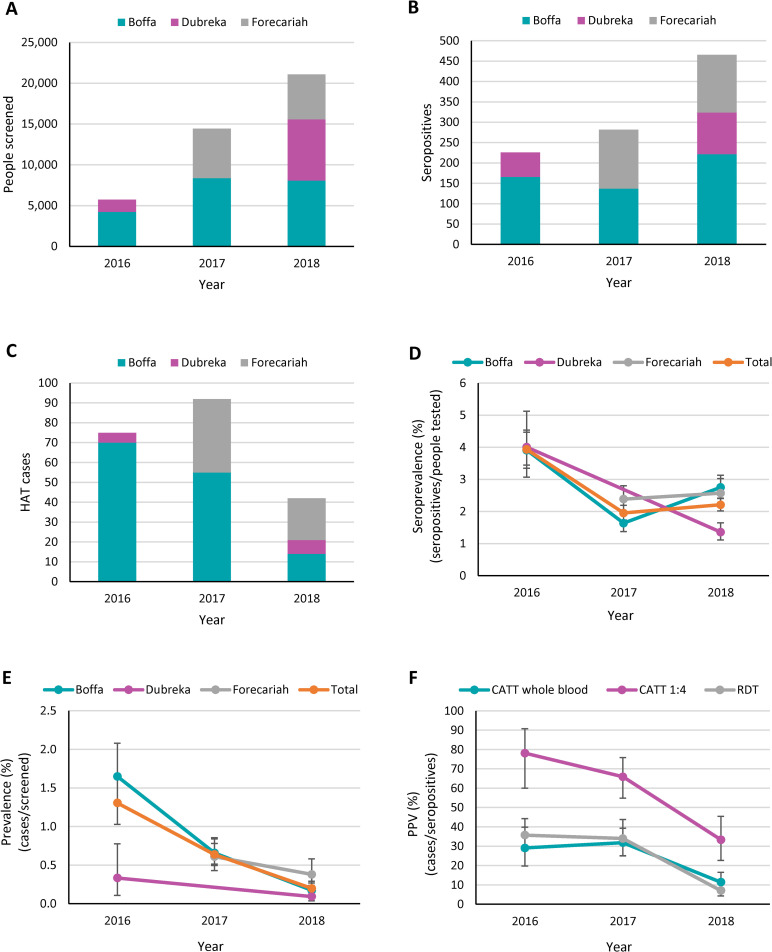
Methodology/principal findings: A retrospective analysis was performed to evaluate the medical activities that were implemented in the three most endemic prefectures of Guinea (Boffa, Dubreka and Forecariah) between January 2016 and December 2018. Passive screening using rapid diagnostic tests (RDTs) was progressively resumed in one hundred and one health facilities, and active screening was intensified by visiting individual households and performing RDTs, and by conducting mass screening in villages by mobile teams using the Card Agglutination Test for Trypanosomiasis. A total of 1885, 4897 and 8023 clinical suspects were tested in passive, while 5743, 14442 and 21093 people were actively screened in 2016, 2017 and 2018, respectively. The number of HAT cases that were diagnosed first went up from 107 in 2016 to 140 in 2017, then subsequently decreased to only 73 in 2018. A progressive decrease in disease prevalence was observed in the populations that were tested in active and in passive between 2016 and 2018.
Conclusions/significance: Intensified medical interventions in the post-Ebola context first resulted in an increase in the number of HAT cases, confirming the fear that the disease could resurge as a result of impaired control activities during the Ebola epidemic. On the other hand, the decrease in disease prevalence that was observed between 2016 and 2018 is encouraging, as it suggests that the current strategy combining enhanced diagnosis, treatment and vector control is appropriate to progress towards elimination of HAT in Guinea.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
