

The effect of dexamethasone on sugammadex reversal of rocuronium-induced neuromuscular blockade in surgical patients undergoing general anesthesia: A systematic review and meta-analysis
- PMID: 33592855
- PMCID: PMC7870250
- DOI: 10.1097/MD.0000000000023992
The effect of dexamethasone on sugammadex reversal of rocuronium-induced neuromuscular blockade in surgical patients undergoing general anesthesia: A systematic review and meta-analysis
Abstract
Background: There have been conflicting results regarding clinical dexamethasone-sugammadex interactions in adults and pediatric patients under general anesthesia.
Methods: This study used a systematic review with meta-analysis of randomized controlled trials and non-randomized studies based on the Cochrane Review Methods. A comprehensive literature search was conducted to identify clinical trials that investigated the effect of dexamethasone on sugammadex reversal of rocuronium-induced neuromuscular blockade in surgical patients undergoing general anesthesia.
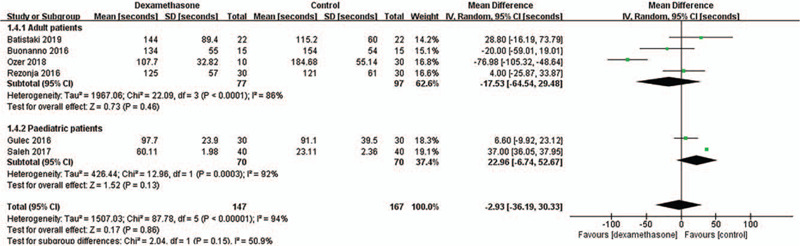
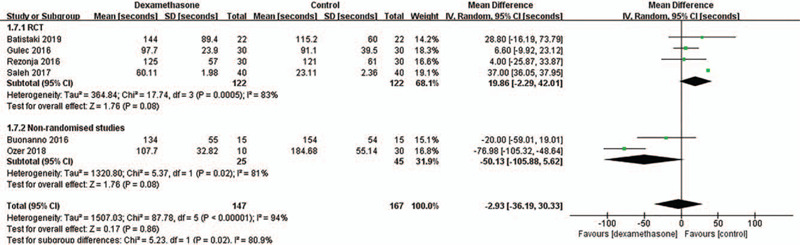
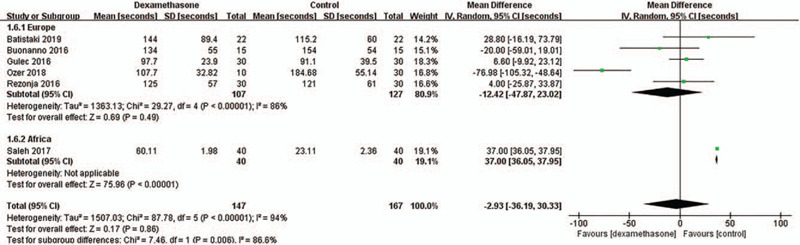
Results: Among the 314 patients in the 6 studies, 147 received intravenous dexamethasone (dexamethasone group), and 167 received intravenous saline or other antiemetics (control group). The primary outcome, the time to recovery after sugammadex administration (the time to recovery of the train-of-four ratio to 0.9 after sugammadex administration; s) was comparable between the 2 groups, the weighted mean difference (95% confidence interval [CI]) being -2.93 (-36.19, 30.33) (I2 = 94%). The time to extubation after sugammadex administration (s) and incidence of postoperative nausea and vomiting was not different between the 2 groups, the weighted mean difference (95% CI) being 23.31 (-2.26, 48.88) (I2 = 86%) and the pooled risk ratio (95% CI) being 0.25 (0.03, 2.11), respectively. The time to recovery after sugammadex administration might be different according to the study design or study region.
Conclusion: This meta-analysis showed that use of dexamethasone in the perioperative period neither delayed nor facilitated the reversal of rocuronium-induced neuromuscular blockade with sugammadex in patients undergoing elective surgery with general anesthesia. However, given that the results showed high heterogeneity, further randomized controlled trials are needed to confirm these findings.
Copyright © 2021 the Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
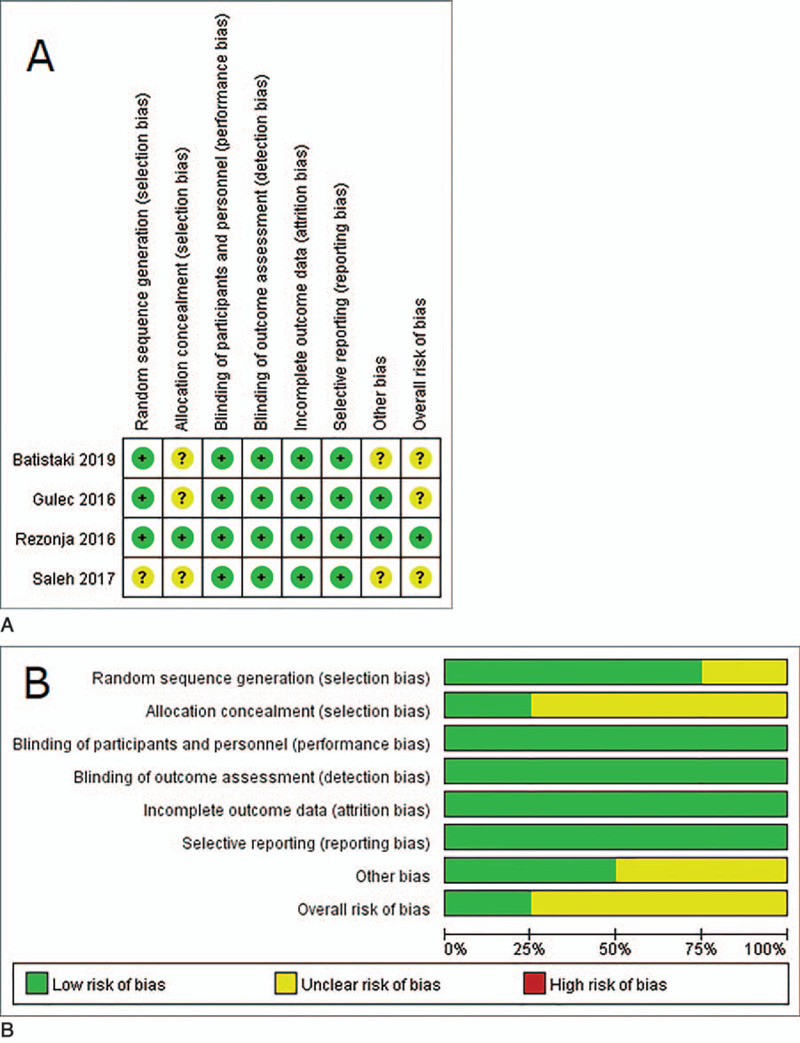
Figures



References
-
- Gijsenbergh F, Ramael S, Houwing N, et al. First human exposure of Org 25969, a novel agent to reverse the action of rocuronium bromide. Anesthesiology 2005;103:695–703. - PubMed
-
- Kovac AL. Sugammadex: the first selective binding reversal agent for neuromuscular block. J Clin Anesth 2009;21:444–53. - PubMed
-
- Rezonja K, Sostaric M, Vidmar G, et al. Dexamethasone produces dose-dependent inhibition of sugammadex reversal in in vitro innervated primary human muscle cells. Anesth Analg 2014;118:755–63. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
