

Feasibility, effectiveness, and safety of endoscopic vacuum therapy for intrathoracic anastomotic leakage following transthoracic esophageal resection
- PMID: 33593301
- PMCID: PMC7885467
- DOI: 10.1186/s12876-021-01651-6
Feasibility, effectiveness, and safety of endoscopic vacuum therapy for intrathoracic anastomotic leakage following transthoracic esophageal resection
Abstract
Background: Anastomotic leakage (AL) in the upper gastrointestinal (GI) tract is associated with high morbidity and mortality rates. Especially intrathoracic anastomotic leakage leads to life-threatening complications. Endoscopic vacuum therapy (EVT) for anastomotic leakage after transthoracic esophageal resection represents a novel concept. However, sound clinical data are still scarce. This retrospective, single-center study aimed to evaluate the feasibility, effectiveness, and safety of EVT for intrathoracic anastomotic leakage following abdomino-thoracic esophageal resection.
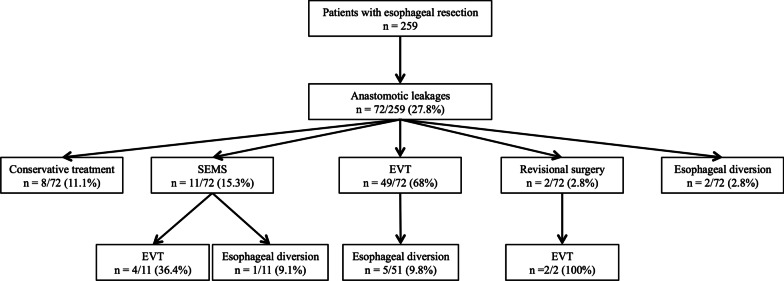
Methods: From March 2014 to September 2019 259 consecutive patients underwent elective transthoracic esophageal resection. 72 patients (27.8%) suffered from AL. The overall collective in-hospital mortality rate was 3.9% (n = 10). Data from those who underwent treatment with EVT were included.
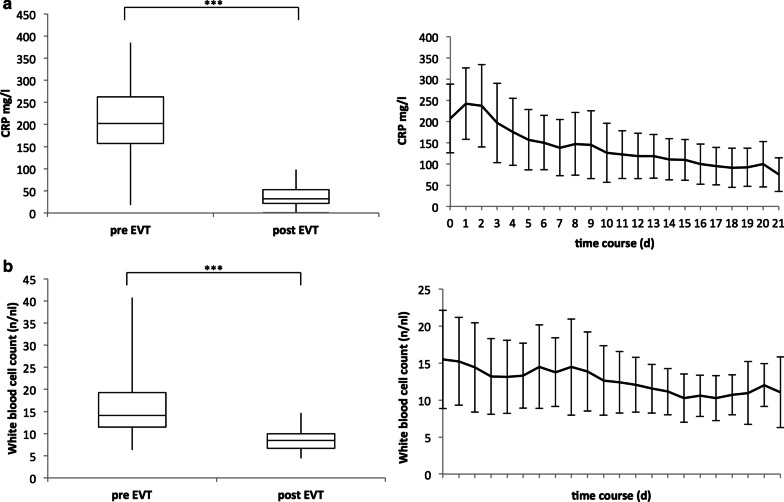
Results: Fifty-five patients were treated with EVT. Successful closure was achieved in 89.1% (n = 49) by EVT only. The EVT-associated complication rate was 5.4% (n = 3): bleeding occurred in one patient, while minor sedation-related complications were observed in two patients. The median number of EVT procedures per patient was 3. The procedures were performed at intervals of 3-5 days, with a 14-day median duration of therapy. The mortality rate of patients with AL was 7.2% (n = 4). Despite successfully terminated EVT, three patients died because of multiple organ failure, acute respiratory distress syndrome, and urosepsis (5.4%). One patient (1.8%) died during EVT due to cardiac arrest.
Conclusions: EVT is a safe and effective approach for intrathoracic anastomotic leakages following abdomino-thoracic esophageal resections. It offers a high leakage-closure rate and the potential to lower leakage-related mortalities.
Trial registration: This trial was registered and approved by the Institutional Ethics Committee of the University of Heidelberg on 16.04.2014 (Registration Number: S-635/2013).
Keywords: Anastomotic leakage; Endoscopic vacuum therapy; Endoscopy; Negative-pressure therapy; Postoperative complications.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
The Optimal Treatment Strategy for Postoperative Anastomotic Leakage After Esophagectomy: a Comparative Analysis Between Endoscopic Vacuum Therapy and Conventional Treatment.J Gastrointest Surg. 2023 Dec;27(12):2899-2906. doi: 10.1007/s11605-023-05637-5. Epub 2023 Dec 1. J Gastrointest Surg. 2023. PMID: 38040922
-
Endoscopic vacuum therapy versus stent treatment of esophageal anastomotic leaks (ESOLEAK): study protocol for a prospective randomized phase 2 trial.Trials. 2021 Jun 2;22(1):377. doi: 10.1186/s13063-021-05315-4. Trials. 2021. PMID: 34078426 Free PMC article.
-
Self-Expanding Metal Stents Versus Endoscopic Vacuum Therapy in Anastomotic Leak Treatment After Oncologic Gastroesophageal Surgery.J Gastrointest Surg. 2019 Jan;23(1):67-75. doi: 10.1007/s11605-018-4000-x. Epub 2018 Oct 29. J Gastrointest Surg. 2019. PMID: 30374816
-
Management of intra-thoracic anastomotic leakages after esophagectomy: updated systematic review and meta-analysis of endoscopic vacuum therapy versus stenting.BMC Surg. 2022 Aug 11;22(1):309. doi: 10.1186/s12893-022-01764-z. BMC Surg. 2022. PMID: 35953796 Free PMC article.
-
Surgical Endoscopic Vacuum-assisted Closure Therapy (EVAC) in Treating Anastomotic Leakages After Major Resective Surgery of Esophageal and Gastric Cancer.Anticancer Res. 2018 Oct;38(10):5581-5587. doi: 10.21873/anticanres.12892. Anticancer Res. 2018. PMID: 30275175 Review.
Cited by
-
Evolution of endoscopic vacuum therapy for upper gastrointestinal leakage over a 10-year period: a quality improvement study.Surg Endosc. 2022 Dec;36(12):9169-9178. doi: 10.1007/s00464-022-09400-w. Epub 2022 Jul 19. Surg Endosc. 2022. PMID: 35852622 Free PMC article.
-
Real-life introduction of powered circular stapler for esophagogastric anastomosis: cohort and propensity matched score study.Dis Esophagus. 2023 Apr 29;36(5):doac073. doi: 10.1093/dote/doac073. Dis Esophagus. 2023. PMID: 36222069 Free PMC article.
-
The Optimal Treatment Strategy for Postoperative Anastomotic Leakage After Esophagectomy: a Comparative Analysis Between Endoscopic Vacuum Therapy and Conventional Treatment.J Gastrointest Surg. 2023 Dec;27(12):2899-2906. doi: 10.1007/s11605-023-05637-5. Epub 2023 Dec 1. J Gastrointest Surg. 2023. PMID: 38040922
-
Applications of endoscopic vacuum therapy in the upper gastrointestinal tract.World J Gastrointest Endosc. 2023 Jun 16;15(6):420-433. doi: 10.4253/wjge.v15.i6.420. World J Gastrointest Endosc. 2023. PMID: 37397978 Free PMC article. Review.
-
Endoscopic Vacuum Therapy for Anastomotic Leakage After Distal Gastrectomy in a Renal Transplant Patient: A Case Study.Am J Case Rep. 2025 May 20;26:e946626. doi: 10.12659/AJCR.946626. Am J Case Rep. 2025. PMID: 40392762 Free PMC article.
References
-
- Alanezi K, Urschel JD. Mortality secondary to esophageal anastomotic leak. Ann Thorac Cardiovasc Surg. 2004;10(2):71–75. - PubMed
-
- Hulscher JB, van Sandick JW, de Boer AG, Wijnhoven BP, Tijssen JG, Fockens P, Stalmeier PF, ten Kate FJ, van Dekken H, Obertop H, et al. Extended transthoracic resection compared with limited transhiatal resection for adenocarcinoma of the esophagus. N Engl J Med. 2002;347(21):1662–1669. - PubMed
-
- Biere SS, van Berge Henegouwen MI, Maas KW, Bonavina L, Rosman C, Garcia JR, Gisbertz SS, Klinkenbijl JH, Hollmann MW, de Lange ES, et al. Minimally invasive versus open oesophagectomy for patients with oesophageal cancer: a multicentre, open-label, randomised controlled trial. Lancet. 2012;379(9829):1887–1892. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
