

Natural course of fat necrosis after breast reconstruction: a 10-year follow-up study
- PMID: 33593330
- PMCID: PMC7885495
- DOI: 10.1186/s12885-021-07881-x
Natural course of fat necrosis after breast reconstruction: a 10-year follow-up study
Abstract
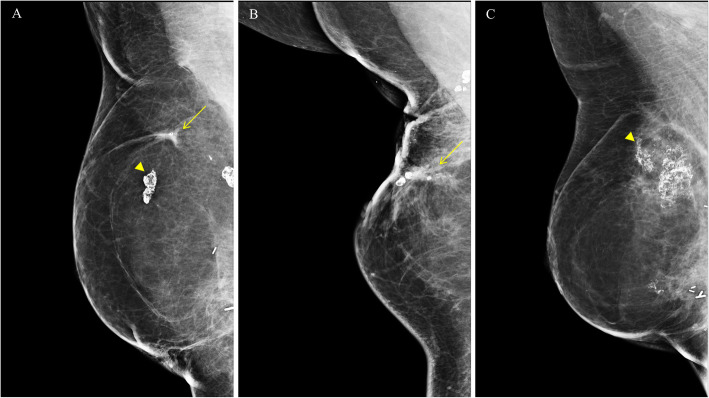
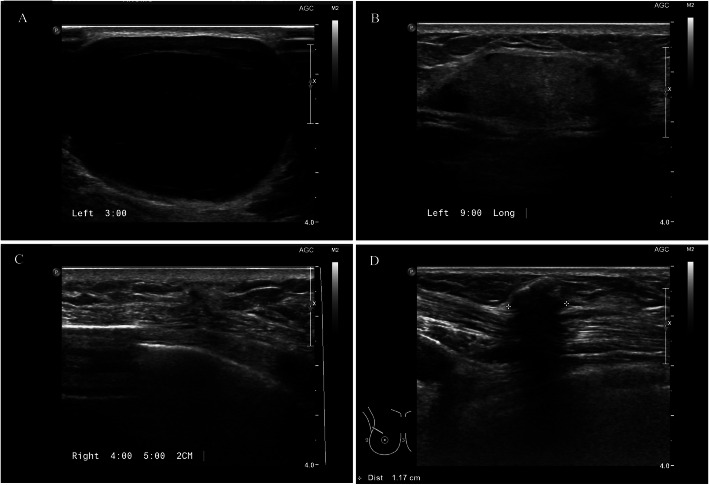
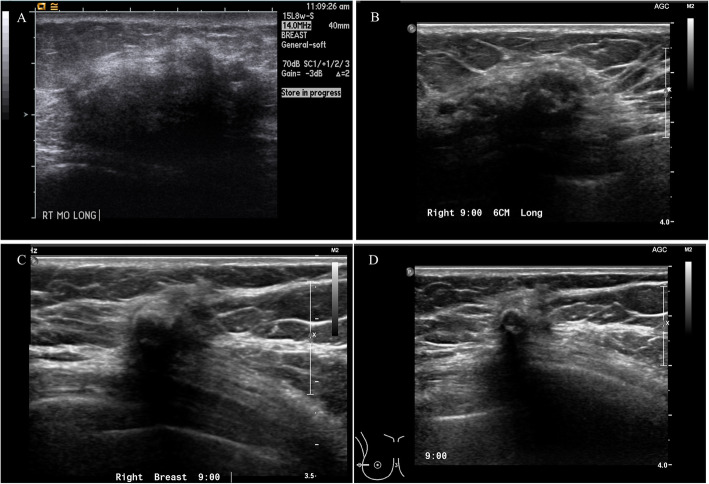
Background: Although fat necrosis is a minor postoperative complication after breast reconstruction, occasionally it mimics to tumor recurrence in patients with breast cancer. Therefore, the surgeon should distinguish between benign fat necrosis and true local recurrence. The authors evaluated the clinical characteristics of fat necrosis after breast reconstruction and investigated the natural course of fat necrosis.
Methods: Between 2007 and 2013, a total of 362 patients underwent breast reconstruction after partial or total mastectomy for breast cancer in Kyungpook National University Hospital. Clinicopathologic characteristics and the occurrence of fat necrosis were assessed during surveillance for 10 years of mean follow-up period.
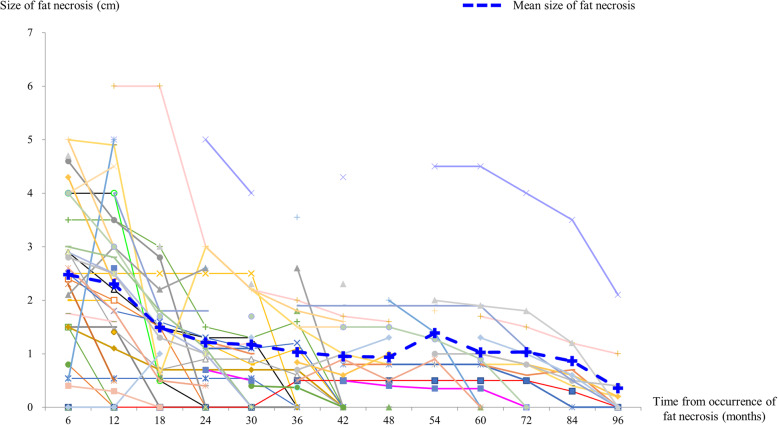
Results: There were 42 cases (11.6%) of fat necrosis after breast reconstruction with partial or total mastectomy which were confirmed by needle or excision biopsy. The fat necrosis was resolved after a mean period of 45.9 months (SD, ± 42.1) and 26 cases (61.9%) of fat necrosis were almost completely resolved (less than 5 mm) during 10-year follow-up period.
Conclusion: Based on the natural course of fat necrosis, the fat necrosis after breast reconstruction can be only monitored, if pathologic confirmation was done. More than half of the cases will be resolved within 2-3 years.
Keywords: Breast; Breast reconstruction; Carcinoma; Fat necrosis.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Outcomes of Autologous Fat Grafting in Mastectomy Patients Following Breast Reconstruction.Ann Surg Oncol. 2018 Oct;25(10):3052-3056. doi: 10.1245/s10434-018-6597-0. Epub 2018 Jul 2. Ann Surg Oncol. 2018. PMID: 29968032
-
Autologous Fat Grafting After Breast Reconstruction in Postmastectomy Patients: Complications, Biopsy Rates, and Locoregional Cancer Recurrence Rates.Ann Plast Surg. 2016 Mar;76(3):270-5. doi: 10.1097/SAP.0000000000000561. Ann Plast Surg. 2016. PMID: 26101979
-
Fat necrosis in level I oncoplastic breast-conserving surgery focusing on a modified round block technique.Breast Cancer. 2020 Jul;27(4):567-572. doi: 10.1007/s12282-020-01046-7. Epub 2020 Jan 13. Breast Cancer. 2020. PMID: 31933122
-
The Use of Tumescent Technique in Mastectomy and Related Complications: A Meta-Analysis.Plast Reconstr Surg. 2019 Jan;143(1):39-48. doi: 10.1097/PRS.0000000000005100. Plast Reconstr Surg. 2019. PMID: 30589774
-
Imaging findings after a total reconstructed breast with autologous fat transfer: what the radiologist needs to know.BJR Open. 2024 Apr 24;6(1):tzae010. doi: 10.1093/bjro/tzae010. eCollection 2024 Jan. BJR Open. 2024. PMID: 38798692 Free PMC article. Review.
Cited by
-
Using ICG to Streamline Perforator Selection in DIEP Flap Reconstruction: Retrospective cohort study of outcomes in our first one hundred flaps.JPRAS Open. 2025 Mar 6;44:331-338. doi: 10.1016/j.jpra.2025.02.016. eCollection 2025 Jun. JPRAS Open. 2025. PMID: 40276248 Free PMC article.
-
Forgotten Surgical Sponge Mimicking Fat Necrosis Following Breast Reduction Surgery.Plast Reconstr Surg Glob Open. 2025 Jul 22;13(7):e7007. doi: 10.1097/GOX.0000000000007007. eCollection 2025 Jul. Plast Reconstr Surg Glob Open. 2025. PMID: 40698271 Free PMC article.
-
Tissue perfusion in DIEP flaps using Indocyanine Green Fluorescence Angiography, Hyperspectral imaging, and Thermal imaging.JPRAS Open. 2024 May 1;41:61-74. doi: 10.1016/j.jpra.2024.04.007. eCollection 2024 Sep. JPRAS Open. 2024. PMID: 38948075 Free PMC article.
References
-
- WP. A. Surgery of the breast: principles and art. edition. S, editor. Philadelphia: Lippincott Williams & Wilkins; 2006.
MeSH terms
Grants and funding
- 2014R1A5A2009242, 2019R1F1A1063853/Ministry of National Defense (KR)
- 1420040/National R&D Program for Cancer Control, Ministry of Health and Welfare, Republic of Korea
- HI17C1142/Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea
- NRF-2019R1A2C1006264/National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT)
- 2017M3A9G8083382/National Research Foundation of Korea (NRF) grant funded by the Korea government
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
