

Identification of subgroup effect with an individual participant data meta-analysis of randomised controlled trials of three different types of therapist-delivered care in low back pain
- PMID: 33593341
- PMCID: PMC7885433
- DOI: 10.1186/s12891-021-04028-8
Identification of subgroup effect with an individual participant data meta-analysis of randomised controlled trials of three different types of therapist-delivered care in low back pain
Abstract
Background: Proven treatments for low back pain, at best, only provide modest overall benefits. Matching people to treatments that are likely to be most effective for them may improve clinical outcomes and makes better use of health care resources.
Methods: We conducted an individual participant data meta-analysis of randomised controlled trials of three types of therapist delivered interventions for low back pain (active physical, passive physical and psychological treatments). We applied two statistical methods (recursive partitioning and adaptive risk group refinement) to identify potential subgroups who might gain greater benefits from different treatments from our individual participant data meta-analysis.
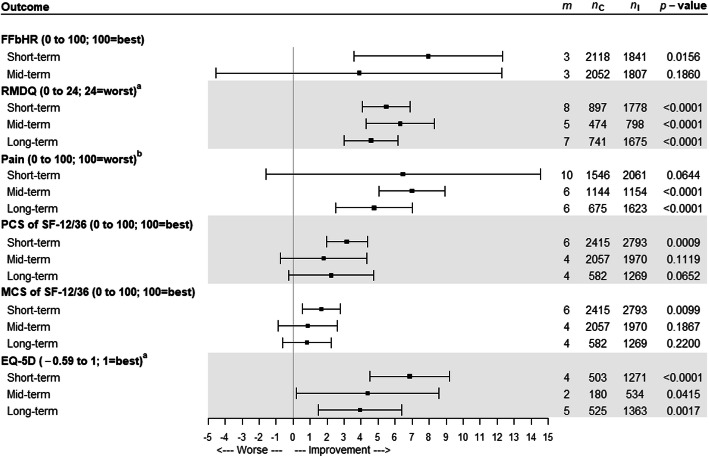
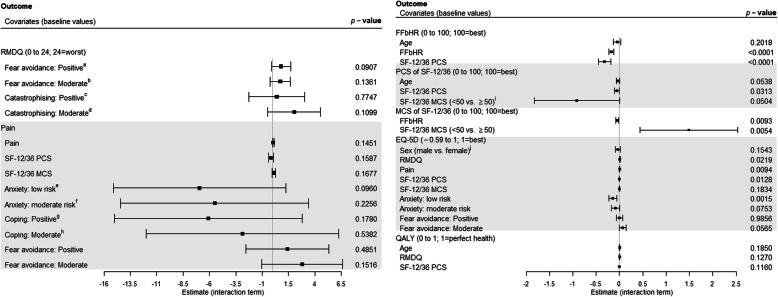
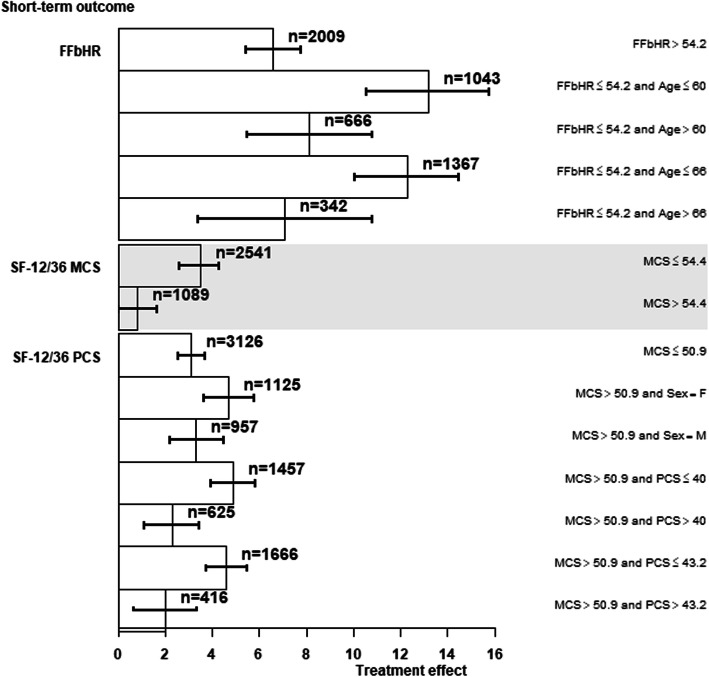
Results: We pooled data from 19 randomised controlled trials, totalling 9328 participants. There were 5349 (57%) females with similar ratios of females in control and intervention arms. The average age was 49 years (standard deviation, SD, 14). Participants with greater psychological distress and physical disability gained most benefit in improving on the mental component scale (MCS) of SF-12/36 from passive physical treatment than non-active usual care (treatment effects, 4.3; 95% confidence interval, CI, 3.39 to 5.15). Recursive partitioning method found that participants with worse disability at baseline gained most benefit in improving the disability (Roland Morris Disability Questionnaire) outcome from psychological treatment than non-active usual care (treatment effects, 1.7; 95% CI, 1.1 to 2.31). Adaptive risk group refinement did not find any subgroup that would gain much treatment effect between psychological and non-active usual care. Neither statistical method identified any subgroups who would gain an additional benefit from active physical treatment compared to non-active usual care.
Conclusions: Our methodological approaches worked well and may have applicability in other clinical areas. Passive physical treatments were most likely to help people who were younger with higher levels of disability and low levels of psychological distress. Psychological treatments were more likely to help those with severe disability. Despite this, the clinical importance of identifying these subgroups is limited. The sizes of sub-groups more likely to benefit and the additional effect sizes observed are small. Our analyses provide no evidence to support the use of sub-grouping for people with low back pain.
Keywords: IPD; Low back pain; Physical interventions; Psychological interventions; Stratification; Subgroups; Therapist delivered interventions.
Conflict of interest statement
MU is chief investigator or co-investigator on multiple previous and current research grants from the UK National Institute for Health Research, Arthritis Research UK and is a co-investigator on grants funded by the Australian NHMRC. He is an NIHR Senior Investigator. He has received travel expenses for speaking at conferences from the professional organisations hosting the conferences. He is a director and shareholder of Clinvivo Ltd. that provides electronic data collection for health services research. He is part of an academic partnership with Serco Ltd. related to return to work initiatives. He is a co-investigator two NIHR funded grants receiving support in kind from Styrker Ltd. He was until March 2020 an editor of the NIHR journal series, and a member of the NIHR Journal Editors Group, for which he received a fee. He has published multiple papers on low back pain some of which are referenced in this paper. He was corresponding author for the UK BEAM trial that is included in the database.
SP is a director of Health Psychology Services Ltd. that provides psychological treatments for a range of conditions.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
