

A prospective cohort study evaluating screening and assessment of six modifiable risk factors in HPB cancer patients and compliance to recommended prehabilitation interventions
- PMID: 33593437
- PMCID: PMC7887817
- DOI: 10.1186/s13741-020-00175-z
A prospective cohort study evaluating screening and assessment of six modifiable risk factors in HPB cancer patients and compliance to recommended prehabilitation interventions
Abstract
Introduction: Despite improvements in perioperative care, major abdominal surgery continues to be associated with significant perioperative morbidity. Accurate preoperative risk stratification and optimisation (prehabilitation) are necessary to reduce perioperative morbidity. This study evaluated the screening and assessment of modifiable risk factors amendable for prehabilitation interventions and measured the patient compliance rate with recommended interventions.
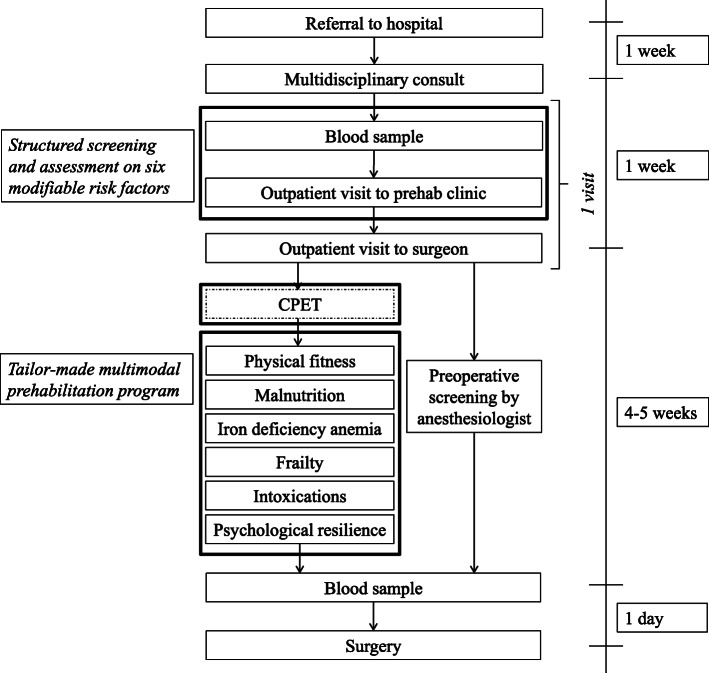
Method: Between May 2019 and January 2020, patients referred to our hospital for HPB surgery were screened and assessed on six modifiable preoperative risk factors. The risk factors and screening tools used, with cutoff values, included (i) low physical fitness (a 6-min walk test < 82% of patient's calculated norm and/or patient's activity level not meeting the global recommendations on physical activity for health). Patients who were unfit based on the screening were assessed with a cardiopulmonary exercise test (anaerobic threshold ≤ 11 mL/kg/min); (ii) malnutrition (patient-generated subjective global assessment ≥ 4); (iii) iron-deficiency anaemia (haemoglobin < 12 g/dL for women, < 13 g/dL for men and transferrin saturation ≤ 20%); (iv) frailty (Groningen frailty indicator/Robinson frailty score ≥ 4); (v) substance use (smoking and alcohol use of > 5 units per week) and (vi) low psychological resilience (Hospital Anxiety and Depression Scale ≥ 8). Patients had a consultation with the surgeon on the same day as their screening. High-risk patients were referred for necessary interventions.
Results: One hundred consecutive patients were screened at our prehabilitation outpatient clinic. The prevalence of high-risk patients per risk factor was 64% for low physical fitness, 42% for malnutrition, 32% for anaemia (in 47% due to iron deficiency), 22% for frailty, 12% for smoking, 18% for alcohol use and 21% for low psychological resilience. Of the 77 patients who were eventually scheduled for surgery, 53 (68.8%) needed at least one intervention, of whom 28 (52.8%) complied with 100% of the necessary interventions. The median (IQR) number of interventions needed in the 77 patients was 1.0 (0-2).
Conclusion: It is feasible to screen and assess all patients referred for HPB cancer surgery for six modifiable risk factors. Most of the patients had at least one risk factor that could be optimised. However, compliance with the suggested interventions remains challenging.
Keywords: Prehabilitation; Preoperative care pathway; Risk stratification; Screening.
Conflict of interest statement
The authors declare no competing interests
Figures
Similar articles
-
Treatment of iron deficiency in patients scheduled for pancreatic surgery: implications for daily prehabilitation practice in pancreatic surgery.Perioper Med (Lond). 2023 Jul 11;12(1):36. doi: 10.1186/s13741-023-00323-1. Perioper Med (Lond). 2023. PMID: 37434251 Free PMC article.
-
Personalized multimodal prehabilitation reduces cardiopulmonary complications after pancreatoduodenectomy: results of a propensity score matching analysis.HPB (Oxford). 2023 Nov;25(11):1429-1437. doi: 10.1016/j.hpb.2023.07.899. Epub 2023 Jul 25. HPB (Oxford). 2023. PMID: 37558563
-
Prehabilitation for Hepatopancreatobiliary Surgical Patients: Interim Analysis Demonstrates a Protective Effect From Neoadjuvant Chemotherapy and Improvement in the Frailty Phenotype.Am Surg. 2021 May;87(5):714-724. doi: 10.1177/0003134820952378. Epub 2020 Nov 10. Am Surg. 2021. PMID: 33170023 Clinical Trial.
-
Staging the Host: Personalizing Risk Assessment for Radical Cystectomy Patients.Eur Urol Oncol. 2018 Sep;1(4):292-304. doi: 10.1016/j.euo.2018.05.010. Epub 2018 Jun 19. Eur Urol Oncol. 2018. PMID: 31100250 Review.
-
Exercise and Nutrition Interventions for Prehabilitation in Hepato-Pancreato-Biliary Cancers: A Narrative Review.Nutrients. 2023 Dec 8;15(24):5044. doi: 10.3390/nu15245044. Nutrients. 2023. PMID: 38140303 Free PMC article. Review.
Cited by
-
Impact of Preoperative Diabetes Mellitus on Postoperative Outcomes in Elective Pancreatic Surgery and Its Implications for Prehabilitation Practice.Pancreas. 2024 Mar 1;53(3):e274-e279. doi: 10.1097/MPA.0000000000002300. Epub 2024 Jan 26. Pancreas. 2024. PMID: 38277400 Free PMC article.
-
Understanding Patients' Experiences and Perspectives of Tele-Prehabilitation: A Qualitative Study to Inform Service Design and Delivery.Clin Pract. 2022 Aug 16;12(4):640-652. doi: 10.3390/clinpract12040067. Clin Pract. 2022. PMID: 36005070 Free PMC article.
-
Prognostic factor in patient with recurrent pancreatic adenocarcinoma.Langenbecks Arch Surg. 2023 Sep 2;408(1):347. doi: 10.1007/s00423-023-03073-2. Langenbecks Arch Surg. 2023. PMID: 37658871
-
Inter-rater variability for the American Society of Anesthesiologists classification in patients undergoing hepato-pancreato-biliary surgery (MILESTONE-2): international survey among surgeons and anaesthesiologists.BJS Open. 2024 Dec 30;9(1):zrae162. doi: 10.1093/bjsopen/zrae162. BJS Open. 2024. PMID: 40036750 Free PMC article.
-
Multimodal prehabilitation in patients with non-small cell lung cancer: a feasibility study.J Thorac Dis. 2024 May 31;16(5):2776-2789. doi: 10.21037/jtd-23-1929. Epub 2024 May 10. J Thorac Dis. 2024. PMID: 38883662 Free PMC article.
References
-
- Barberan-Garcia A, Ubre M, Pascual-Argente N, et al. Post-discharge impact and cost-consequence analysis of prehabilitation in high-risk patients undergoing major abdominal surgery: secondary results from a randomised controlled trial. Br J Anaesth. 2019;123(4):450–456. doi: 10.1016/j.bja.2019.05.032. - DOI - PubMed
-
- Berkel AEM, Bongers BC, van Kamp MS, et al. The effects of prehabilitation versus usual care to reduce postoperative complications in high-risk patients with colorectal cancer or dysplasia scheduled for elective colorectal resection: study protocol of a randomized controlled trial. BMC Gastroenterol. 2018;18(1):29–26. doi: 10.1186/s12876-018-0754-6. - DOI - PMC - PubMed
-
- Berkel AEM, Van Wijk L, Bongers BC, Van Der Palen J, Buis CI, Reudink M, Liem MSL, Slooter GD, Van Meeteren NLU, Klaase JM. Study protocol of a single-arm pre-post study to assess the preliminary effectiveness and feasibility of a home-based bimodal prehabilitation program on preoperative aerobic fitness in high-risk patients scheduled for liver or pancreatic resection. Int J Clin Trials. 2020;7(2):103–111. doi: 10.18203/2349-3259.ijct20201716. - DOI
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
