

The Role of Dexmedetomidine as an Additive to Intravenous Regional Anesthesia: A Systematic Review and Meta-analysis
- PMID: 33593724
- PMCID: PMC8880966
- DOI: 10.5152/balkanmedj.2021.20076
The Role of Dexmedetomidine as an Additive to Intravenous Regional Anesthesia: A Systematic Review and Meta-analysis
Abstract
Background: Intravenous Regional Anesthesia (IVRA) is a reliable and cost-effective anesthetic method for minor surgical procedures to the extremities. Limitations of this block include tourniquet discomfort, short duration of anesthesia, and absence of postoperative analgesia. Dexmedetomidine has been used as an adjuvant to minimize these negative characteristics with inconclusive results.
Aim: To perform a systematic review of the existing evidence on the role of dexmedetomidine as an additive to intravenous regional anesthesia in upper limb surgery.
Study design: Systematic Review and Meta-analysis.
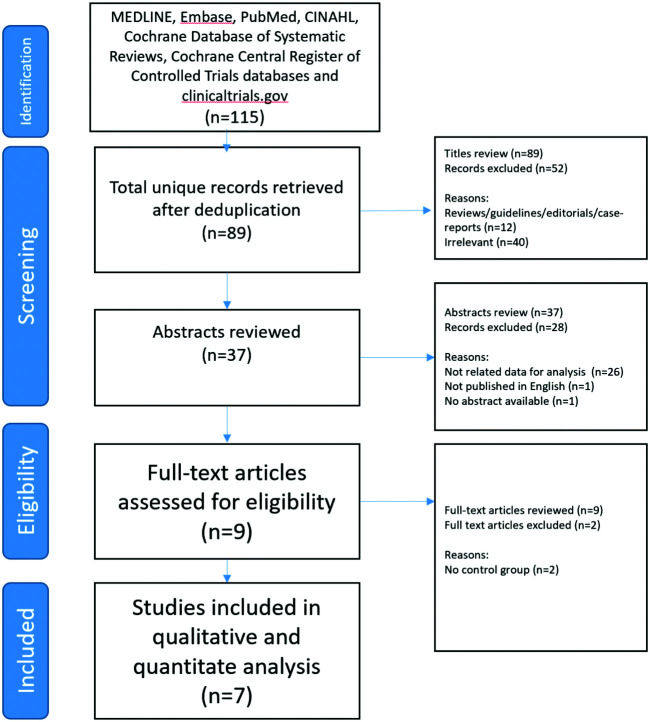
Methods: The databases searched were MEDLINE, Embase, PubMed, CINAHL, Cochrane Database of Systematic Reviews, Cochrane Central Register of Controlled Trials databases, and clinicaltrials. gov (1990-2019). Seven randomized controlled trials (RCTs) were included. We analyzed the duration of analgesia, onset time of sensory and motor block, intraoperative tourniquet pain scores, the incidence of tourniquet pain, need for rescue analgesia, intraoperative rescue analgesia consumption, sedation scores, postoperative pain scores, and anesthesia quality.
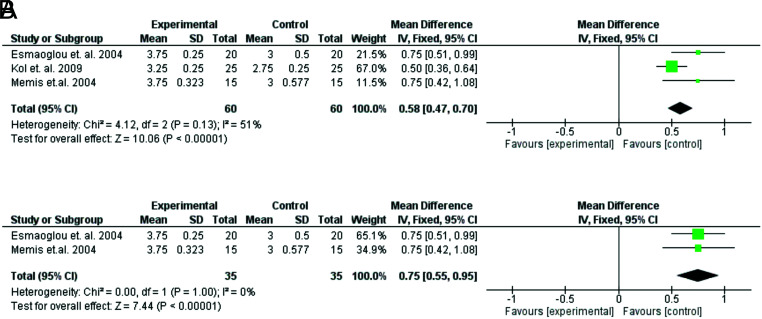
Results: Intraoperative analgesia duration (MD 11.08 min; 95% CI 5.42, 16.75; P < .0001) was longer and sensory block onset time (MD -2.10 min; 95% CI -3.345, -0.86; P = .00009) was shorter in the dexmedetomidine group. Anesthesia quality scores (MD 0.58; 95% CI 0.47, 0.70; P < .00001) and postoperative sedation scores (MD 1.03; 95% CI 0.88, 1.24; P < .00001) were significantly higher. There was a significant reduction in intraoperative rescue analgesia consumption (MD -19.70 mg; 95% CI -24.15, -15.26; P < .00001) in the dexmedetomidine group. The risk of tourniquet pain as well as postoperative pain scores were lower in favor of dexmedetomidine. The addition of dexmedetomidine to IVRA slightly increased the risk of sedation. A limitation of our study is that some of the interesting outcomes derive from a small number of RCTs.
Conclusion: The addition of dexmedetomidine to IVRA ameliorates the block's characteristics and carries a low risk of potential side effects.
Figures





References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources