

Direct oral anticoagulants in treatment of cerebral venous thrombosis: a systematic review
- PMID: 33593766
- PMCID: PMC7888326
- DOI: 10.1136/bmjopen-2020-040212
Direct oral anticoagulants in treatment of cerebral venous thrombosis: a systematic review
Abstract
Objectives: Current guidelines do not recommend direct oral anticoagulants (DOACs) to treat cerebral venous thrombosis (CVT) despite their benefits over standard therapy. We performed a systematic review to summarise the published experience of DOAC therapy in CVT.
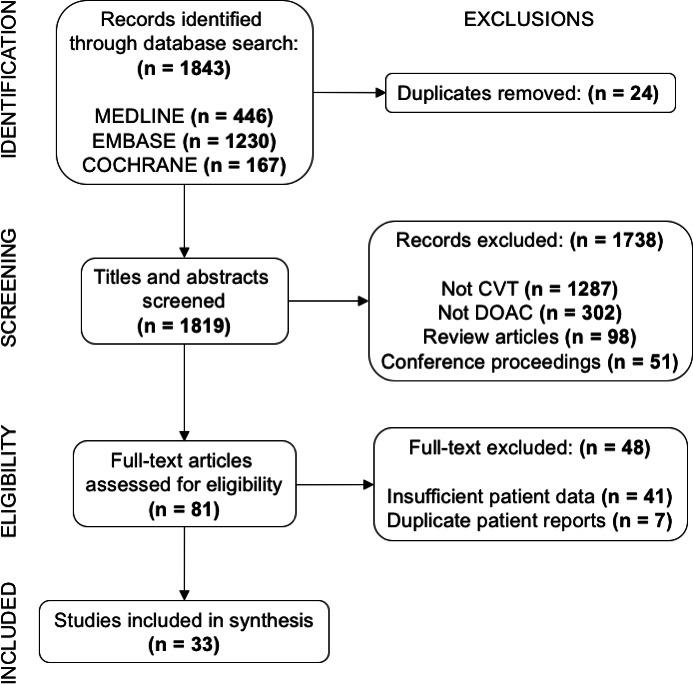
Data sources: MEDLINE, Embase and COCHRANE databases up to 18 November 2020.
Eligibility criteria: All published articles of patients with CVT treated with DOAC were included. Studies without follow-up information were excluded.
Data extraction and synthesis: Two independent reviewers screened articles and extracted data. A risk of bias analysis was performed.
Primary and secondary outcome measures: Safety data included mortality, intracranial haemorrhage (ICH) or other adverse events. Efficacy data included recurrent CVT, recanalisation rates and disability by modified Rankin Scales (mRS).
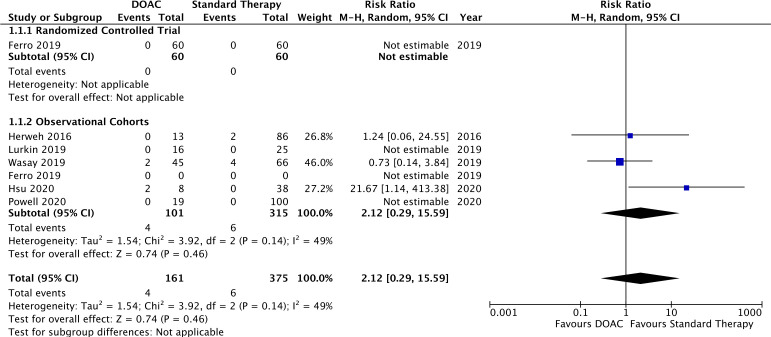
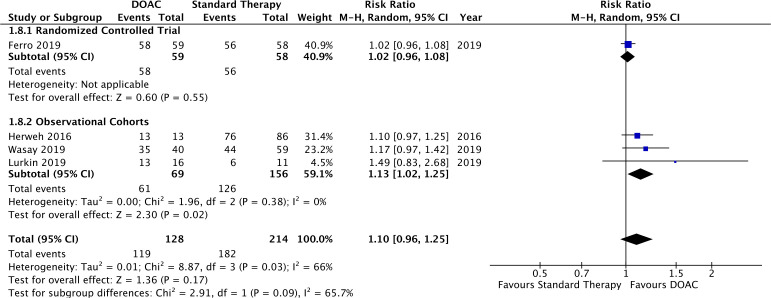
Results: 33 studies met inclusion criteria. One randomised controlled trial, 5 observational cohorts and 27 case series or studies reported 279 patients treated with DOAC for CVT: 41% dabigatran, 47% rivaroxaban, 10% apixaban and 2% edoxaban, in addition to 315 patients treated with standard therapy. The observational cohorts showed a similar risk of death in DOAC and standard therapy arms (RR 2.12, 95% CI 0.29 to 15.59). New ICH was reported in 2 (0.7%) DOAC-treated patients and recurrent CVT occurred in 4 (1.5%). A favourable mRS between 0 and 2 was reported in 94% of DOAC-treated patients, more likely than standard therapy in observational cohorts (RR 1.13, 95% CI 1.02 to 1.25).
Conclusion: The evidence for DOAC use in CVT is limited although suggests sufficient safety and efficacy despite variability in timing and dose of treatment. This systematic review highlights that further rigorous trials are needed to validate these findings and to determine optimal treatment regimens.
Keywords: anticoagulation; epidemiology; stroke; stroke medicine.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: GB: none. JG: none. VY: none. RS: none. DAF: none. GLG holds an Early Researcher Award from the Ontario Ministry of Research and Innovation (MRI); an Ontario Mid-Career Investigator Award from the Heart and Stroke Foundation of Canada; and a University of Ottawa, Faculty of Medicine Tier 1 Clinical Research Chair in Diagnosis of Venous Thromboembolism. He has indirectly received research funding from Portola, Boehringer-Ingelheim, Pfizer, Bristol-Myers Squibb, LEO Pharma, Daiichi Sankyo, Bayer. He has received speaker honoraria from Bayer, Pfizer, LEO Pharma, Sanofi bioMérieux. JC: has received research funding from the following non-profit organisations: Dutch Heart Foundation, Dutch Brain Foundation and Amsterdam Neuroscience. He has also received research support from Bayer, Boehringer and Portola. All fees were paid to his institute and used to fund medical research. MM: none. MV-B received speaker fees from Boehringer Ingelheim, Portugal, is part of an advisory board of Daiichi Sankyo, Portugal, and received a travel grant from Boehringer Ingelheim, Portugal. SN: received consulting fees from Brainomix and Böhringer Ingelheim and Honoria for lectures from Bayer, BMS Pfizer and Medtronic. DD received a Heart & Stroke Foundation of Canada Clinician Scientist Award, and has received honoraria from Bayer, BMS and Apopharma.
Figures
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous