

Molecular Signatures of Inflammatory Profile and B-Cell Function in Patients with Severe Fever with Thrombocytopenia Syndrome
- PMID: 33593977
- PMCID: PMC8545090
- DOI: 10.1128/mBio.02583-20
Molecular Signatures of Inflammatory Profile and B-Cell Function in Patients with Severe Fever with Thrombocytopenia Syndrome
Abstract
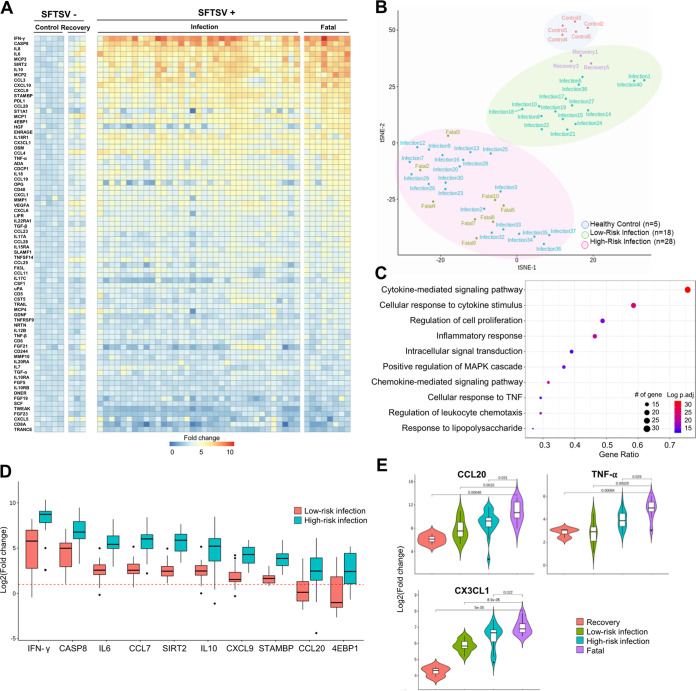
Dabie bandavirus (severe fever with thrombocytopenia syndrome virus [SFTSV]) induces an immunopathogenic disease with a high fatality rate; however, the mechanisms underlying its clinical manifestations are largely unknown. In this study, we applied targeted proteomics and single-cell transcriptomics to examine the differential immune landscape in SFTS patient blood. Serum immunoprofiling identified low-risk and high-risk clusters of SFTS patients based on inflammatory cytokine levels, which corresponded to disease severity. Single-cell transcriptomic analysis of SFTS patient peripheral blood mononuclear cells (PBMCs) at different infection stages showed pronounced expansion of B cells with alterations in B-cell subsets in fatal cases. Furthermore, plasma cells in which the interferon (IFN) pathway is downregulated were identified as the primary reservoir of SFTSV replication. This study identified not only the molecular signatures of serum inflammatory cytokines and B-cell lineage populations in SFTSV-induced fatalities but also plasma cells as the viral reservoir. Thus, this suggests that altered B-cell function is linked to lethality in SFTSV infections.IMPORTANCE SFTSV is an emerging virus discovered in China in 2009; it has since spread to other countries in East Asia. Although the fatality rates of SFTSV infection range from 5.3% to as high as 27%, the mechanisms underlying clinical manifestations are largely unknown. In this study, we demonstrated that SFTSV infection in fatal cases caused an excessive inflammatory response through high induction of proinflammatory cytokines and chemokines and the aberrant inactivation of adaptive immune responses. Furthermore, single-cell transcriptome sequencing (RNA-seq) analysis of SFTS patient PBMCs revealed that SFTSV targets the B-cell lineage population, especially plasma cells, as the potential viral reservoir in patients for whom the infection is fatal. Thus, SFTSV infection may inhibit high-affinity antibody maturation and secretion of plasma B cells, suppressing neutralizing antibody production and thereby allowing significant virus replication and subsequent fatality.
Keywords: SFTS; SFTSV; bandavirus; emerging virus; immunoprofiling; plasma B cell; proximity extension assay; single-cell RNA-seq.
Copyright © 2021 Park et al.
Figures




References
-
- National Institute of Infectious Diseases. 2019. Severe fever with thrombocytopenia syndrome (SFTS) in Japan, as of June 2019. Infect Agents Surveill Rep 40:111–112.
-
- KCDA. 2020. Infectious Disease Portal. http://www.cdc.go.kr/npt/biz/npp/ist/bass/bassDissStatsMain.do.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
