

Classification of brain arteriovenous malformations located in motor-related areas based on location and anterior choroidal artery feeding
- PMID: 33593985
- PMCID: PMC8485233
- DOI: 10.1136/svn-2020-000591
Classification of brain arteriovenous malformations located in motor-related areas based on location and anterior choroidal artery feeding
Abstract
Objective: Surgical management of arteriovenous malformations (AVMs) involving motor cortex or fibre tracts (M-AVMs) is challenging. This study aimed to construct a classification system based on nidus locations and anterior choroidal artery (AChA) feeding to pre-surgically evaluate motor-related and seizure-related outcomes in patients undergoing resection of M-AVMs.
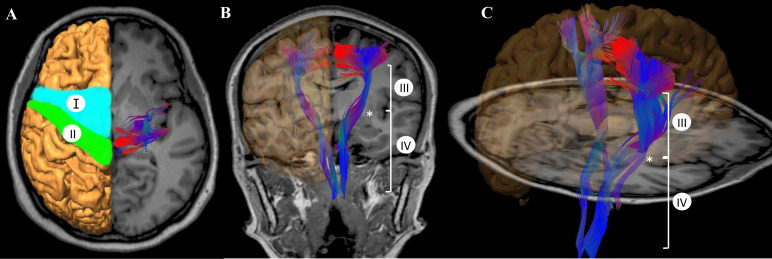
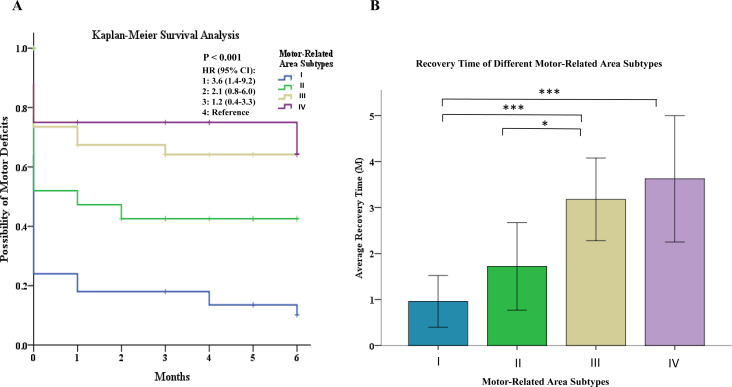
Methods and materials: A total of 125 patients who underwent microsurgical resection of M-AVMs were retrospectively reviewed. Four subtypes were identified based on nidus location: (I) nidus involving the premotor area and/or supplementary motor areas; (II) nidus involving the precentral gyrus; (III) nidus involving the corticospinal tract (CST) and superior to the posterior limb of the internal capsule; (IV) nidus involving the CST at or inferior to the level of posterior limb of the internal capsule. In addition, we divided type IV into type IVa and type IVb according to the AChA feeding. Surgical-related motor deficit (MD) evaluations were performed 1 week (short-term) and 6 months (long-term) after surgery.
Results: The type I patients exhibited the highest incidence (62.0%) of pre-surgical epilepsy among the four subtypes. Multivariate analysis showed that motor-related area subtypes (p=0.004) and diffuse nidus (p=0.014) were significantly associated with long-term MDs. Long-term MDs were significantly less frequent in type I than in the other types. Type IV patients acquired the highest proportion (four patients, 25.0%) of long-term poor outcomes (mRS >2). Type IVb patients showed a significantly higher incidence of post-surgical MDs than type IVa patients (p=0.041). The MDs of type III or IV patients required more recovery time. Of the 62 patients who had pre-surgical seizures, 90.3% (56/62) controlled their seizures well and reached Engel class I after surgery.
Conclusions: Combining the consideration of location and AChA feeding, the classification for M-AVMs is a useful approach for predicting post-surgical motor function and decision-making.
Keywords: arteriovenous malformation.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous