

Modelling safe protocols for reopening schools during the COVID-19 pandemic in France
- PMID: 33594076
- PMCID: PMC7887250
- DOI: 10.1038/s41467-021-21249-6
Modelling safe protocols for reopening schools during the COVID-19 pandemic in France
Abstract
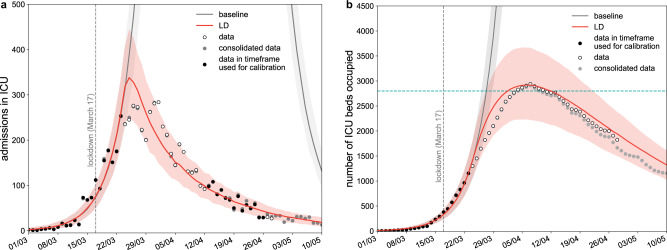
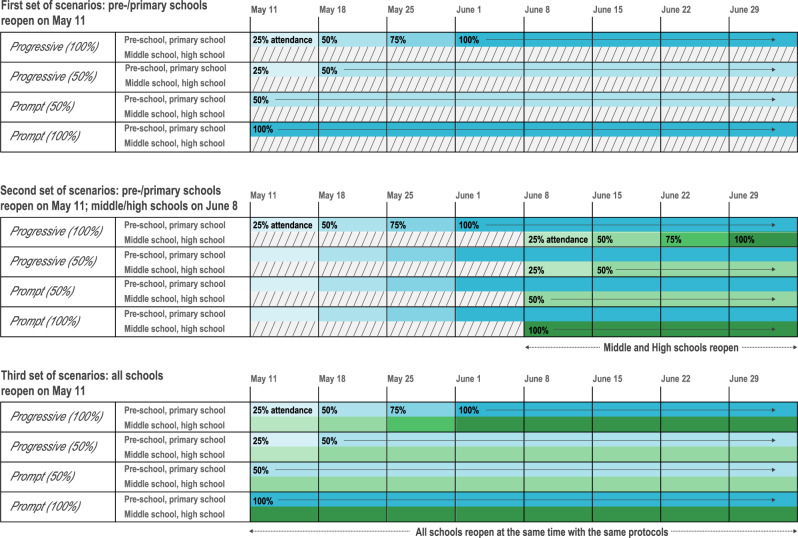
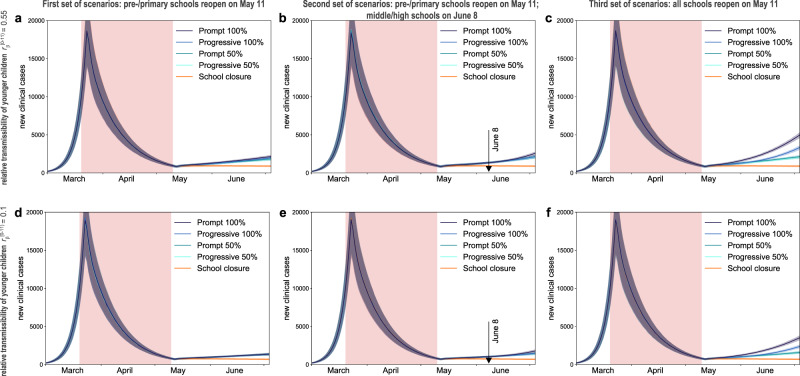
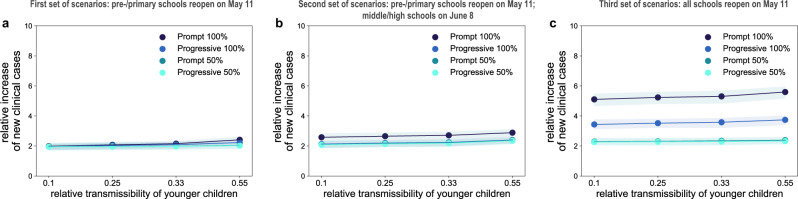
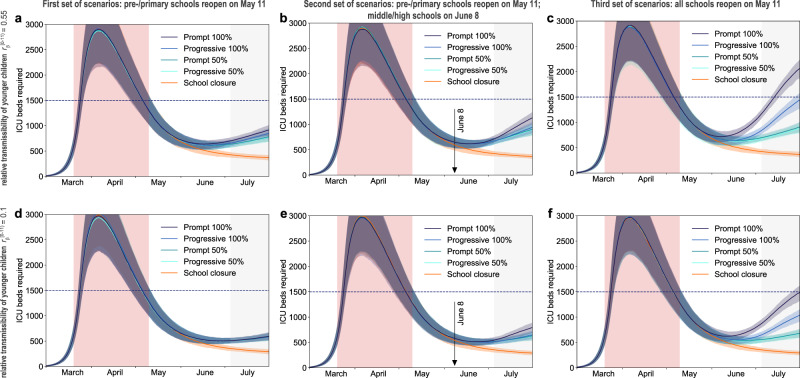
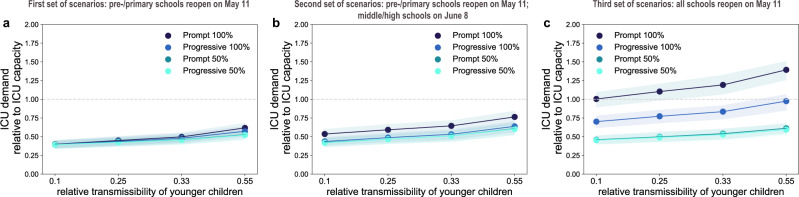
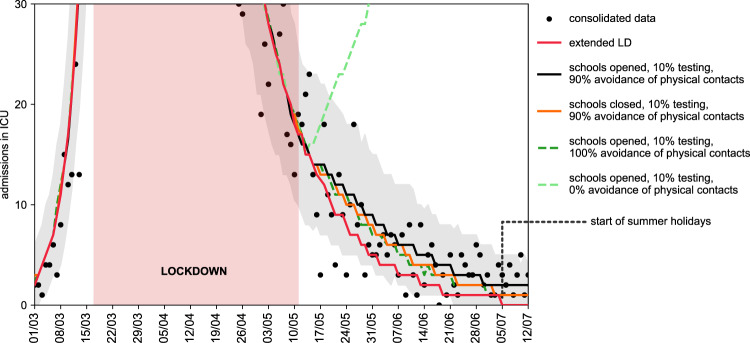
As countries in Europe implement strategies to control the COVID-19 pandemic, different options are chosen regarding schools. Through a stochastic age-structured transmission model calibrated to the observed epidemic in Île-de-France in the first wave, we explored scenarios of partial, progressive, or full school reopening. Given the uncertainty on children's role, we found that reopening schools after lockdown may increase COVID-19 cases, yet protocols exist to keep the epidemic controlled. Under a scenario with stable epidemic activity if schools were closed, reopening pre-schools and primary schools would lead to up to 76% [67, 84]% occupation of ICU beds if no other school level reopened, or if middle and high schools reopened later. Immediately reopening all school levels may overwhelm the ICU system. Priority should be given to pre- and primary schools allowing younger children to resume learning and development, whereas full attendance in middle and high schools is not recommended for stable or increasing epidemic activity. Large-scale test and trace is required to keep the epidemic under control. Ex-post assessment shows that progressive reopening of schools, limited attendance, and strong adoption of preventive measures contributed to a decreasing epidemic after lifting the first lockdown.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- European Centre for Disease Prevention and Control. COVID-19 in Children and the Role of School Settings in Transmission-First Update. https://www.ecdc.europa.eu/sites/default/files/documents/COVID-19-in-chi... (2020).
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
