

Enabling a learning healthcare system with automated computer protocols that produce replicable and personalized clinician actions
- PMID: 33594410
- PMCID: PMC8661391
- DOI: 10.1093/jamia/ocaa294
Enabling a learning healthcare system with automated computer protocols that produce replicable and personalized clinician actions
Abstract
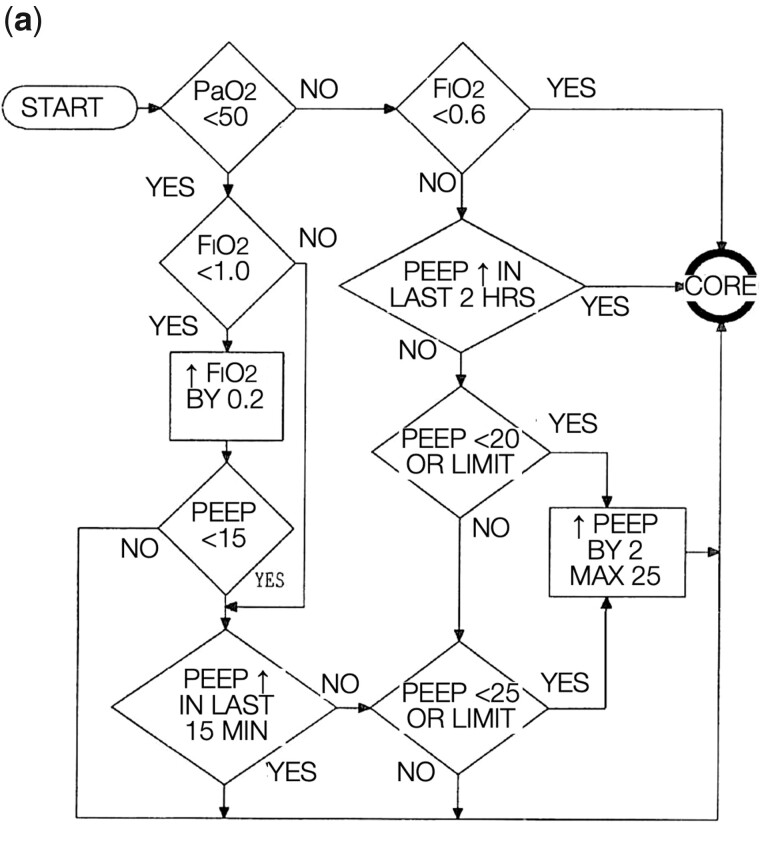
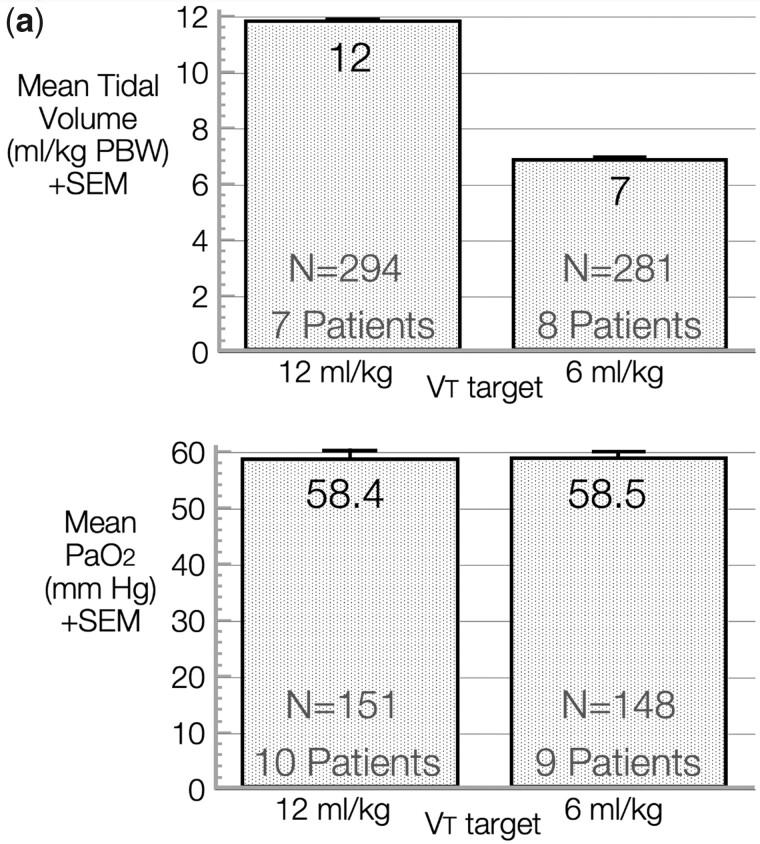
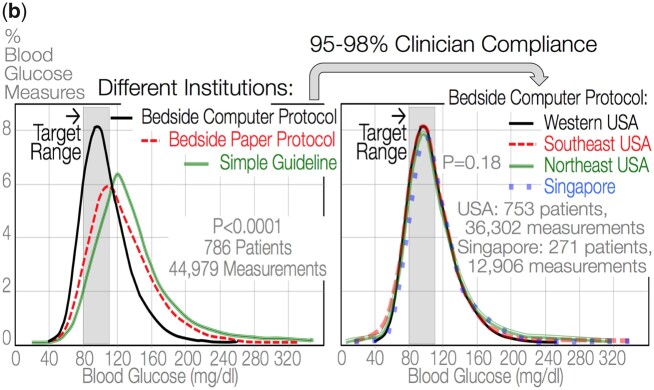
Clinical decision-making is based on knowledge, expertise, and authority, with clinicians approving almost every intervention-the starting point for delivery of "All the right care, but only the right care," an unachieved healthcare quality improvement goal. Unaided clinicians suffer from human cognitive limitations and biases when decisions are based only on their training, expertise, and experience. Electronic health records (EHRs) could improve healthcare with robust decision-support tools that reduce unwarranted variation of clinician decisions and actions. Current EHRs, focused on results review, documentation, and accounting, are awkward, time-consuming, and contribute to clinician stress and burnout. Decision-support tools could reduce clinician burden and enable replicable clinician decisions and actions that personalize patient care. Most current clinical decision-support tools or aids lack detail and neither reduce burden nor enable replicable actions. Clinicians must provide subjective interpretation and missing logic, thus introducing personal biases and mindless, unwarranted, variation from evidence-based practice. Replicability occurs when different clinicians, with the same patient information and context, come to the same decision and action. We propose a feasible subset of therapeutic decision-support tools based on credible clinical outcome evidence: computer protocols leading to replicable clinician actions (eActions). eActions enable different clinicians to make consistent decisions and actions when faced with the same patient input data. eActions embrace good everyday decision-making informed by evidence, experience, EHR data, and individual patient status. eActions can reduce unwarranted variation, increase quality of clinical care and research, reduce EHR noise, and could enable a learning healthcare system.
© The Author(s) 2021. Published by Oxford University Press on behalf of the American Medical Informatics Association. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Figures


References
-
- Berwick DM. Era 3 for medicine and health care. JAMA 2016; 315 (13): 1329–30. - PubMed
-
- Stanovich KE. What Intelligence Tests Miss: The Psychology of Rational Thought. New Haven, CT: Yale University Press; 2009: xv, 308.
-
- Henrich JP. The WEIRDest People in the World: How the West Became Psychologically Peculiar and Particularly Prosperous. New York: Farrar, Straus and Giroux; 2020.
-
- Bernard S, James B, Bayley KB. Cost of Poor Quality or Waste in Integrated Delivery System Settings. Agency for Healthcare research and Quality: RTI International; 2006 September 2006. Report No.: AHRQ Publication No. 08-0096-EF Contract No.: RTI Project No. 0207897.011.
-
- Diamond GA, Pollock BH, Work JW.. Clinician decisions and computers. J Am Coll Cardiol 1987; 9 (6): 1385–96. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
