

Low Back Pain and Substance Use: Diagnostic and Administrative Coding for Opioid Use and Dependence Increased in U.S. Older Adults with Low Back Pain
- PMID: 33594426
- PMCID: PMC8599750
- DOI: 10.1093/pm/pnaa428
Low Back Pain and Substance Use: Diagnostic and Administrative Coding for Opioid Use and Dependence Increased in U.S. Older Adults with Low Back Pain
Abstract
Objective: Low back pain (LBP) is a leading cause of pain and disability. Substance use complicates the management of LBP, and potential risks increase with aging. Despite implications for an aging, diverse U.S. population, substance use and LBP comorbidity remain poorly defined. The objective of this study was to characterize LBP and substance use diagnoses in older U.S. adults by age, gender, and race.
Design: Cross-sectional study of a random national sample.
Subjects: Older adults including 1,477,594 U.S. Medicare Part B beneficiaries.
Methods: Bayesian analysis of 37,634,210 claims, with 10,775,869 administrative and 92,903,649 diagnostic code assignments.
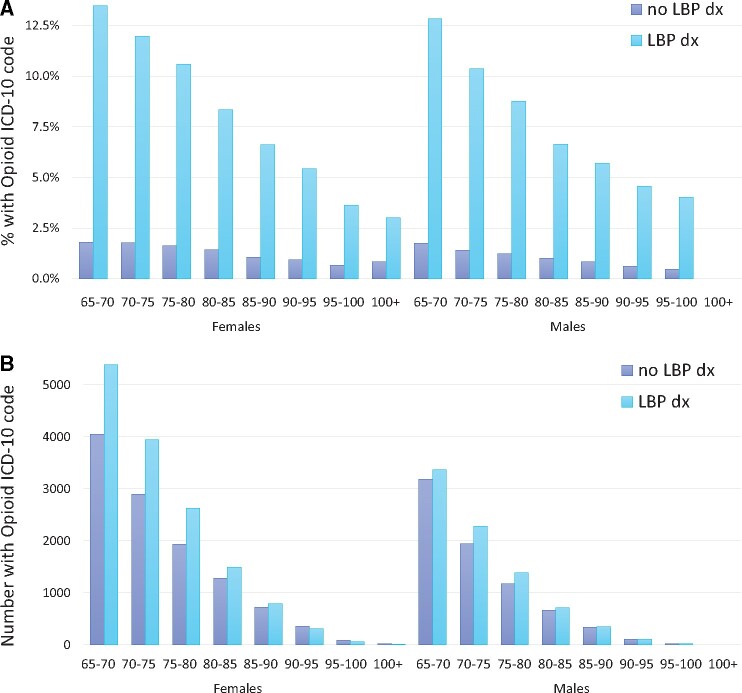
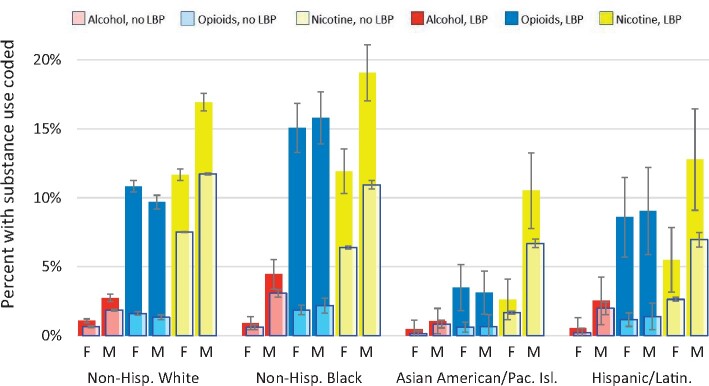
Results: LBP was diagnosed in 14.8±0.06% of those more than 65 years of age, more in females than in males (15.8±0.08% vs. 13.4±0.09%), and slightly less in those more than 85 years of age (13.3±0.2%). Substance use diagnosis varied by substance: nicotine, 9.6±0.02%; opioid, 2.8±0.01%; and alcohol, 1.3±0.01%. Substance use diagnosis declined with advancing age cohort. Opioid use diagnosis was markedly higher for those in whom LBP was diagnosed (10.5%) than for those not diagnosed with LBP (1.5%). Most older adults (54.9%) with an opioid diagnosis were diagnosed with LBP. Gender differences were modest. Relative rates of substance use diagnoses in LBP were modest for nicotine and alcohol.
Conclusions: Older adults with LBP have high relative rates of opioid diagnoses, irrespective of gender or age. Most older adults with opioid-related diagnoses have LBP, compared with a minority of those not opioid diagnosed. In caring for older adults with LBP or opioid-related diagnoses, health systems must anticipate complexity and support clinicians, patients, and caregivers in managing pain comorbidities. Older adults may benefit from proactive incorporation of non-opioid pain treatments. Further study is needed.
Keywords: Addiction; Aging; Alcohol; Gender Differences; Geriatrics; Low Back Pain; Nicotine; Opioids; Pain; Substance Use Disorders.
Published by Oxford University Press on behalf of the American Academy of Pain Medicine. This work is written by a US Government employee and is in the public domain in the US.
Figures

Similar articles
-
Opioid Use in Adults With Low Back or Lower Extremity Pain Who Undergo Spine Surgical Treatment Within 1 Year of Diagnosis.Spine (Phila Pa 1976). 2020 Dec 15;45(24):1725-1735. doi: 10.1097/BRS.0000000000003663. Spine (Phila Pa 1976). 2020. PMID: 32833930
-
The incidence, providers involved, and patient factors associated with diagnosis of specific lumbar spine pathology subsequent an initial nonspecific low back pain diagnosis.Spine J. 2025 Apr;25(4):688-695. doi: 10.1016/j.spinee.2024.10.008. Epub 2024 Nov 4. Spine J. 2025. PMID: 39505011
-
Association of Patient Race and Ethnicity With Differences in Opioid Prescribing by Primary Care Physicians for Older Adults With New Low Back Pain.JAMA Health Forum. 2021 Sep 10;2(9):e212333. doi: 10.1001/jamahealthforum.2021.2333. eCollection 2021 Sep. JAMA Health Forum. 2021. PMID: 35977182 Free PMC article.
-
Harms and benefits of opioids for management of non-surgical acute and chronic low back pain: a systematic review.Br J Sports Med. 2020 Jun;54(11):664. doi: 10.1136/bjsports-2018-099805. Epub 2019 Mar 22. Br J Sports Med. 2020. PMID: 30902816
-
Medications for Treating Low Back Pain in Adults. Evidence for the Use of Paracetamol, Opioids, Nonsteroidal Anti-inflammatories, Muscle Relaxants, Antibiotics, and Antidepressants: An Overview for Musculoskeletal Clinicians.J Orthop Sports Phys Ther. 2022 Jul;52(7):425-431. doi: 10.2519/jospt.2022.10788. Epub 2022 May 18. J Orthop Sports Phys Ther. 2022. PMID: 35584029 Review.
Cited by
-
Prevalence and predictors of musculoskeletal health complaints among sedentary, monotonous urban workers: A survey in Bangladesh.PLoS One. 2023 Apr 21;18(4):e0282922. doi: 10.1371/journal.pone.0282922. eCollection 2023. PLoS One. 2023. PMID: 37083655 Free PMC article.
-
Pain, comorbidities, and clinical decision-making: conceptualization, development, and pilot testing of the Pain in Aging, Educational Assessment of Need instrument.Front Pain Res (Lausanne). 2024 Feb 22;5:1254792. doi: 10.3389/fpain.2024.1254792. eCollection 2024. Front Pain Res (Lausanne). 2024. PMID: 38455875 Free PMC article.
-
Pain when it "counts": hurdle analysis of clinical pain ratings improves data model performance.Pain Rep. 2025 Aug 7;10(5):e1322. doi: 10.1097/PR9.0000000000001322. eCollection 2025 Oct. Pain Rep. 2025. PMID: 40787630 Free PMC article.
-
Multi-Dimensional Impact of Chronic Low Back Pain among Underserved African American and Latino Older Adults.Int J Environ Res Public Health. 2021 Jul 6;18(14):7246. doi: 10.3390/ijerph18147246. Int J Environ Res Public Health. 2021. PMID: 34299695 Free PMC article.
-
Diagnostic rate estimation from Medicare records: Dependence on claim numbers and latent clinical features.J Biomed Inform. 2023 Sep;145:104463. doi: 10.1016/j.jbi.2023.104463. Epub 2023 Jul 28. J Biomed Inform. 2023. PMID: 37517509 Free PMC article.
References
-
- Hoy D, March L, Brooks P, et al.The global burden of low back pain: Estimates from the Global Burden of Disease 2010 study. Ann Rheum Dis 2014;73(6):968–74. - PubMed
-
- U.S. Department of Health and Human Services. Pain Management Best Practices Inter-Agency Task Force Report: Updates, Gaps, Inconsistencies, and Recommendations; 2019. Available at: https://www.hhs.gov/ash/advisory-committees/pain/reports/index.html (accessed March 3, 2020).
-
- Center for Substance Abuse Treatment. Managing Chronic Pain in Adults With or in Recovery From Substance Use Disorders. (SmA) 12-4671. Rockville (MD): Substance Abuse and Mental Health Services Administration (US); 2012. (Treatment Improvement Protocol (TIP) Series, No. 54.) Available at: https://www.ncbi.nlm.nih.gov/books/NBK92048/ (accessed March 3, 2020). - PubMed
-
- Yarnell S, Li L, MacGrory B, Trevisan L, Kirwin P.. Substance use disorders in later life: A review and synthesis of the literature of an emerging public health concern. Am J Geriatr Psychiatry 2020;28(2):226–36. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
