

Outcomes of clinical utility in amyloid-PET studies: state of art and future perspectives
- PMID: 33594474
- PMCID: PMC8175294
- DOI: 10.1007/s00259-020-05187-x
Outcomes of clinical utility in amyloid-PET studies: state of art and future perspectives
Abstract
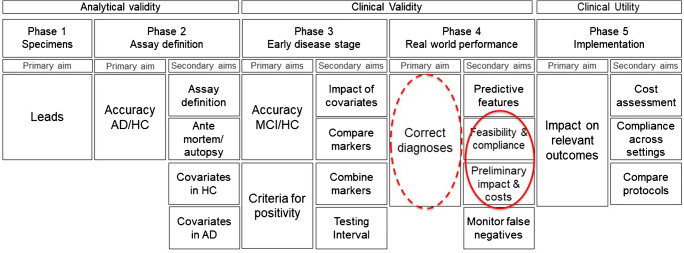
Purpose: To review how outcomes of clinical utility are operationalized in current amyloid-PET validation studies, to prepare for formal assessment of clinical utility of amyloid-PET-based diagnosis.
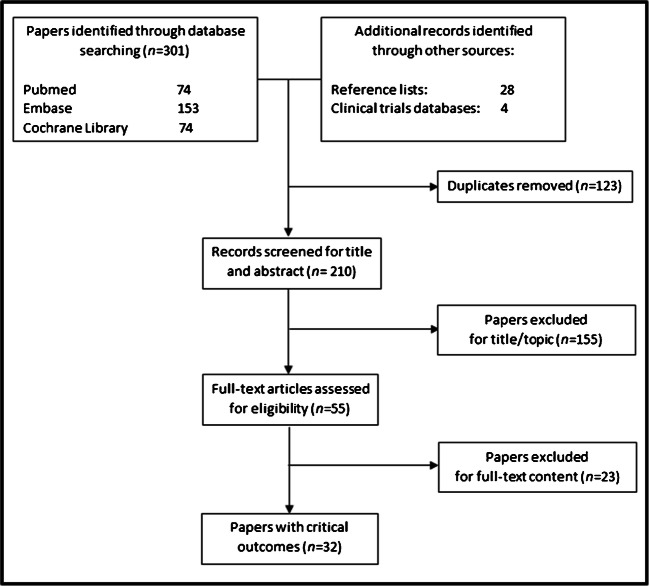
Methods: Systematic review of amyloid-PET research studies published up to April 2020 that included outcomes of clinical utility. We extracted and analyzed (a) outcome categories, (b) their definition, and (c) their methods of assessment.
Results: Thirty-two studies were eligible. (a) Outcome categories were clinician-centered (found in 25/32 studies, 78%), patient-/caregiver-centered (in 9/32 studies, 28%), and health economics-centered (5/32, 16%). (b) Definition: Outcomes were mainly defined by clinical researchers; only the ABIDE study expressly included stakeholders in group discussions. Clinician-centered outcomes mainly consisted of incremental diagnostic value (25/32, 78%) and change in patient management (17/32, 53%); patient-/caregiver-centered outcomes considered distress after amyloid-pet-based diagnosis disclosure (8/32, 25%), including quantified burden of procedure for patients' outcomes (n = 8) (1/8, 12.5%), impact of disclosure of results (6/8, 75%), and psychological implications of biomarker-based diagnosis (75%); and health economics outcomes focused on costs to achieve a high-confidence etiological diagnosis (5/32, 16%) and impact on quality of life (1/32, 3%). (c) Assessment: all outcome categories were operationalized inconsistently across studies, employing 26 different tools without formal rationale for selection.
Conclusion: Current studies validating amyloid-PET already assessed outcomes for clinical utility, although non-clinician-based outcomes were inconsistent. A wider participation of stakeholders may help produce a more thorough and systematic definition and assessment of outcomes of clinical utility and help collect evidence informing decisions on reimbursement of amyloid-PET.
Keywords: Alzheimer’s disease; Amyloid-PET; Clinical utility; Diagnostic biomarkers; Outcome; Systematic review.
Conflict of interest statement
V. Garibotto received financial support for research through her institution from Siemens Healthineers, GE Healthcare, Life Molecular Imaging, Cerveau Technologies, Roche, Merck. G.D. Rabinovici receives research support from the National Institutes of Health, Alzheimer’s Association, American College of Radiology, Rainwater Charitable Foundation, Gift from Edward and Pearl Fein, Avid Radiopharamaceuticals, Eli Lilly, Life Molecular Imaging, GE Healthcare. He has served as a consultant for Axon Neurosciences, Eisai, GE Healthcare, Merck, Genentech. He serves on a data safety monitoring board for Johnson & Johnson. He is an Associate Editor for JAMA Neurology.
F. Barkhof is a member of steering committee and safety monitoring boards for Merck, Biogen and Bayer. He is a consultant for Novartis, Roche, IXICO, GeNeuro, and Combinostics; his institutions received research support from EU/EFPIA Innovative Medicines Initiative Joint Undertaking (EPAD and AMYPAD consortia), Horizon (EuroPOND), UK MS Society, IMDI-NOW (PICTURE), NIHR UCLH Biomedical Research Centre, and ECTRIMS-MAGNIMS. He is section Editor for Neuroradiology. The other authors declare that they have no conflict of interest.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
