

Contribution of P2X4 receptor in pain associated with rheumatoid arthritis: a review
- PMID: 33594635
- PMCID: PMC8155137
- DOI: 10.1007/s11302-021-09764-z
Contribution of P2X4 receptor in pain associated with rheumatoid arthritis: a review
Abstract
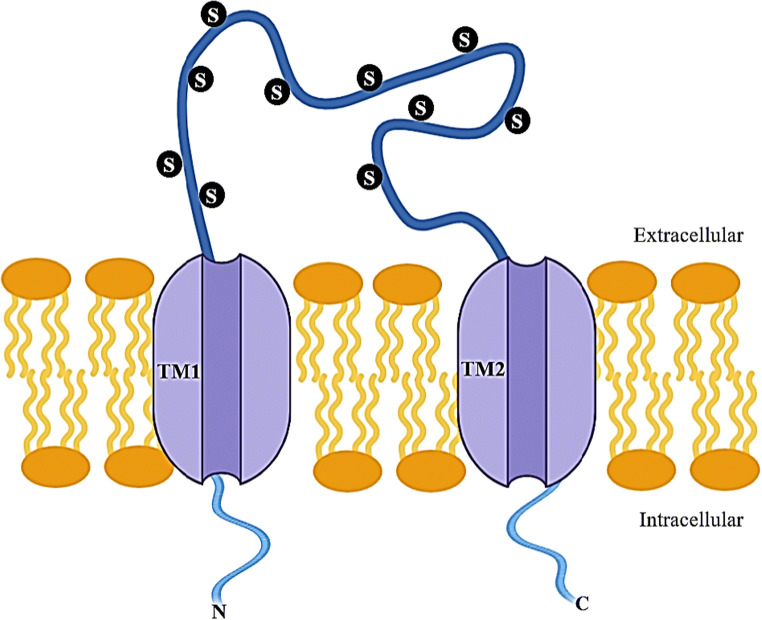
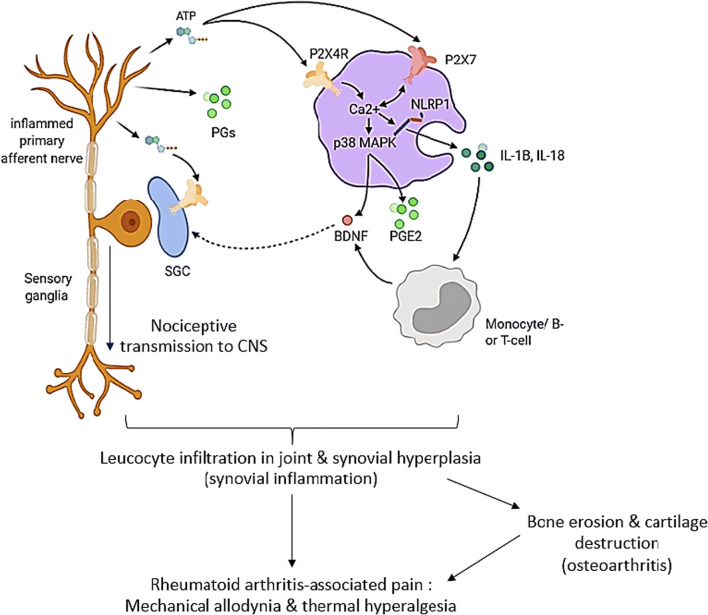
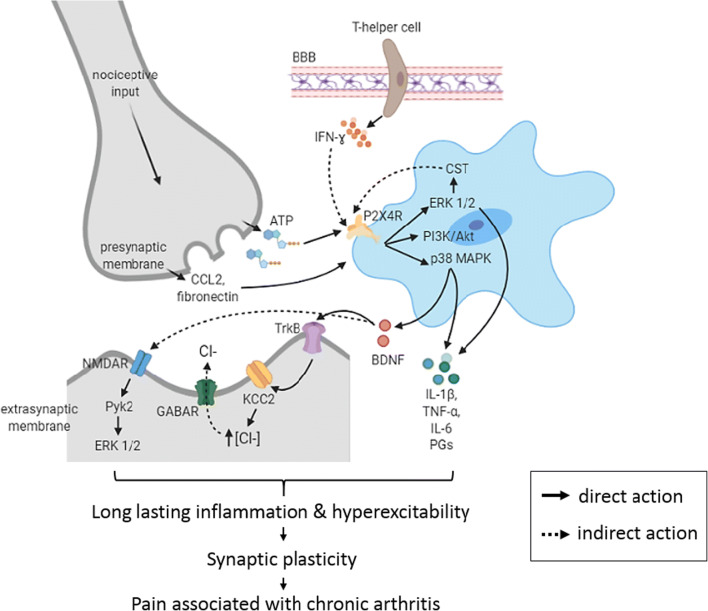
Pain is the most common symptom reported by patients with rheumatoid arthritis (RA) even after the resolution of chronic joint inflammation. It is believed that RA-associated pain is not solely due to inflammation, but could also be attributed to aberrant modifications to the central nervous system. The P2X4 receptor (P2X4R) is an ATP-activated purinergic receptor that plays a significant role in the transmission of information in the nervous system and pain. The involvement of P2X4R during the pathogenesis of chronic inflammatory pain and neuropathic pain is well-established. The attenuation of this receptor alleviates disease pathogenesis and related symptoms, including hyperalgesia and allodynia. Although some studies have revealed the contribution of P2X4R in promoting joint inflammation in RA, how it implicates pain associated with RA at peripheral and central nervous systems is still lacking. In this review, the possible contributions of P2X4R in the nervous system and how it implicates pain transmission and responses were examined.
Keywords: Central pain; Chronic pain; P2X4 receptor; Peripheral pain; Rheumatoid arthritis.
Conflict of interest statement
Nurul Ajilah Mohamed Khir declares that she has no conflict of interest. Ain’ Sabreena Mohd Noh declares that she has no conflict of interest. Nazlahshaniza Shafin declares that she has no conflict of interest. Che Aishah Nazariah Ismail declares that she has no conflict of interest.
Figures
References
-
- Hewlett ST, Sanderson T, May J, Alten R, Bingham CO, III, Cross M, March L, Pohl C, Woodworth T, Bartlett SJ. I’m hurting, I want to kill myself’: rheumatoid arthritis flare is more than a high joint count—an international patient perspective on flare where medical help is sought. Rheumatology. 2012;51(1):69–76. doi: 10.1093/rheumatology/keq455. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
