

What Is the Implant Survivorship and Functional Outcome After Total Humeral Replacement in Patients with Primary Bone Tumors?
- PMID: 33595237
- PMCID: PMC8277276
- DOI: 10.1097/CORR.0000000000001677
What Is the Implant Survivorship and Functional Outcome After Total Humeral Replacement in Patients with Primary Bone Tumors?
Abstract
Background: Total humeral replacement is an option to reconstruct massive bone defects after resection of locally advanced bone tumors of the humerus. However, implant survivorship, potential risk factors for implant revision surgery, and functional results of total humeral replacement are poorly elucidated because of the rarity of the procedure.
Questions/purposes: We asked: (1) What is the revision-free implant and overall limb survivorship after total humerus replacement? (2) What factors are associated with implant revision surgery? (3) What is the functional outcome of the procedure as determined by the Musculoskeletal Tumor Society (MSTS) score and the American Shoulder and Elbow Surgeons (ASES) score?
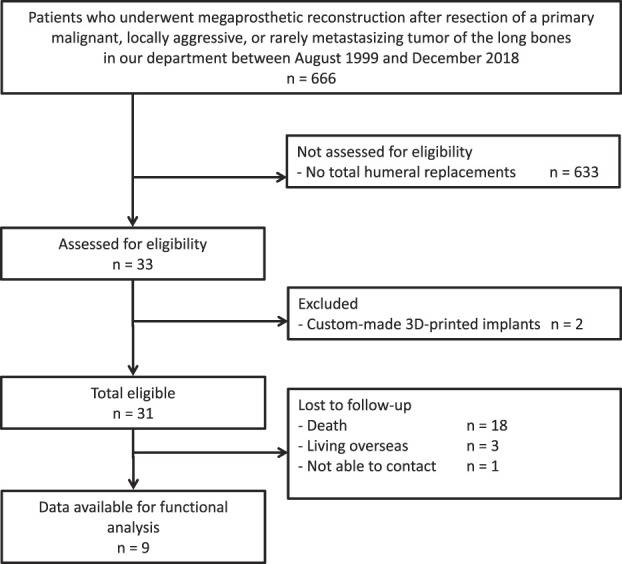
Methods: Between August 1999 and December 2018, 666 patients underwent megaprosthetic reconstruction after resection of a primary malignant or locally aggressive/rarely metastasizing tumor of the long bones at our department. In all, 23% (154) of these patients had a primary tumor located in the humerus. During the study, we performed total humeral replacement in all patients with a locally advanced sarcoma, in patients with pathological fractures, in patients with skip metastases, or in patients with previous intralesional contaminating surgery, who would have no sufficient bone stock for a stable implant fixation for a single joint megaprosthetic replacement of the proximal or distal humerus. We performed no biological reconstructions or reconstructions with allograft-prosthetic composites. As a result, 5% (33 of 666) of patients underwent total humerus replacement. Six percent (2 of 33) of patients were excluded because they received a custom-made, three-dimensionally (3-D) printed hemiprosthesis, leaving 5% (31) of the initial 666 patients for inclusion in our retrospective analysis. Of these, 6% (2 of 31) had surgery more than 5 years ago, but they had not been seen in the last 5 years. Median (interquartile range) age at the time of surgery was 15 years (14 to 25 years), and indications for total humeral replacement were primary malignant bone tumors (n = 30) and a recurring, rarely metastasizing bone tumor (n = 1). All megaprosthetic reconstructions were performed with a single modular system. The implanted prostheses were silver-coated beginning in 2006, and beginning in 2010, a reverse proximal humerus component was used when appropriate. We analyzed endoprosthetic complications descriptively and assessed the functional outcome of all surviving patients who did not undergo secondary amputation using the 1993 MSTS score and the ASES score. The median (IQR) follow-up in all survivors was 75 months (50 to 122 months), with a minimum follow-up period of 25 months. We evaluated the following factors for possible association with implant revision surgery: age, BMI, reconstruction length, duration of surgery, extraarticular resection, pathological fracture, previous intralesional surgery, (neo-)adjuvant radio- and chemotherapy, and metastatic disease.
Results: The revision-free implant survivorship at 1 year was 77% (95% confidence interval 58% to 89%) and 74% (95% CI 55% to 86%) at 5 years. The overall limb survivorship was 93% (95% CI 75% to 98%) after 1 and after 5 years. We found revision-free survivorship to be lower in patients with extraarticular shoulder resection compared with intraarticular resections (50% [95% CI 21% to 74%] versus 89% [95% CI 64% to 97%]) after 5 years (subhazard ratios for extraarticular resections 4.4 [95% CI 1.2 to 16.5]; p = 0.03). With the number of patients available for our analysis, we could not detect a difference in revision-free survivorship at 5 years between patients who underwent postoperative radiotherapy (40% [95% CI 5% to 75%]) and patients who did not (81% [95% CI 60% to 92%]; p = 0.09). The median (IQR) MSTS score in 9 of 13 surviving patients after a median follow-up of 75 months (51 to 148 months) was 87% (67% to 92%), and the median ASES score was 83 (63 to 89) of 100 points, with higher scores representing better function.
Conclusion: Total humeral replacement after resection of locally advanced bone tumors appears to be associated with a good functional outcome in patients who do not die of their tumors, which in our study was approximately one- third of those who were treated with a resection and total humerus prosthesis. However, the probability of early prosthetic revision surgery is high, especially in patients undergoing extraarticular resections, who should be counseled accordingly. Still, our results suggest that if the prosthesis survives the first year, further risk for revision appears to be low. Future studies should reexamine the effect of postoperative radiotherapy on implant survival in a larger cohort and evaluate whether the use of soft tissue coverage with plastic reconstructive surgery might decrease the risk of early revisions, especially in patients undergoing extraarticular resections.
Level of evidence: Level III, therapeutic study.
Copyright © 2021 by the Association of Bone and Joint Surgeons.
Conflict of interest statement
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research® editors and board members are on file with the publication and can be viewed on request.
Figures

Comment in
-
CORR Insights®: What Is the Implant Survivorship and Functional Outcome After Total Humeral Replacement in Patients with Primary Bone Tumors?Clin Orthop Relat Res. 2021 Aug 1;479(8):1765-1767. doi: 10.1097/CORR.0000000000001732. Clin Orthop Relat Res. 2021. PMID: 33739330 Free PMC article. No abstract available.
Similar articles
-
What is the Likelihood That Tumor Endoprostheses Will Experience a Second Complication After First Revision in Patients With Primary Malignant Bone Tumors And What Are Potential Risk Factors?Clin Orthop Relat Res. 2019 Dec;477(12):2705-2714. doi: 10.1097/CORR.0000000000000955. Clin Orthop Relat Res. 2019. PMID: 31764339 Free PMC article.
-
Proximal Humerus Tumors: Higher-than-Expected Risk of Revision With Constrained Reverse Shoulder Arthroplasty.Clin Orthop Relat Res. 2020 Nov;478(11):2585-2595. doi: 10.1097/CORR.0000000000001245. Clin Orthop Relat Res. 2020. PMID: 32281773 Free PMC article.
-
What Is the Survival of the Telescope Allograft Technique to Augment a Short Proximal Femur Segment in Children After Resection and Distal Femur Endoprosthesis Reconstruction for a Bone Sarcoma?Clin Orthop Relat Res. 2021 Aug 1;479(8):1780-1790. doi: 10.1097/CORR.0000000000001686. Clin Orthop Relat Res. 2021. PMID: 33635286 Free PMC article.
-
Causes and Frequencies of Reoperations After Endoprosthetic Reconstructions for Extremity Tumor Surgery: A Systematic Review.Clin Orthop Relat Res. 2019 Apr;477(4):894-902. doi: 10.1097/CORR.0000000000000630. Clin Orthop Relat Res. 2019. PMID: 30801278 Free PMC article.
-
Reconstruction of the elbow with distal humerus endoprosthetic replacement after tumor resection: a systematic review of the literature and institutional case series.J Shoulder Elbow Surg. 2024 May;33(5):1104-1115. doi: 10.1016/j.jse.2023.12.024. Epub 2024 Feb 14. J Shoulder Elbow Surg. 2024. PMID: 38360351
Cited by
-
Comparison of Two Modern Survival Prediction Tools, SORG-MLA and METSSS, in Patients With Symptomatic Long-bone Metastases Who Underwent Local Treatment With Surgery Followed by Radiotherapy and With Radiotherapy Alone.Clin Orthop Relat Res. 2024 Dec 1;482(12):2193-2208. doi: 10.1097/CORR.0000000000003185. Epub 2024 Jul 23. Clin Orthop Relat Res. 2024. PMID: 39051924
-
Does the Duration of Primary and First Revision Surgery Influence the Probability of First and Subsequent Implant Failures after Extremity Sarcoma Resection and Megaprosthetic Reconstruction?Cancers (Basel). 2021 May 21;13(11):2510. doi: 10.3390/cancers13112510. Cancers (Basel). 2021. PMID: 34063771 Free PMC article.
-
The Bateman-Type Soft Tissue Reconstruction around Proximal or Total Humeral Megaprostheses in Patients with Primary Malignant Bone Tumors-Functional Outcome and Endoprosthetic Complications.Cancers (Basel). 2021 Aug 5;13(16):3971. doi: 10.3390/cancers13163971. Cancers (Basel). 2021. PMID: 34439124 Free PMC article.
-
Computer-aided Design and 3D-printed Personalized Stem-plate Composite for Precision Revision of the Proximal Humerus Endoprosthetic Replacement: A Technique Note.Orthop Surg. 2023 Nov;15(11):3000-3005. doi: 10.1111/os.13857. Epub 2023 Sep 18. Orthop Surg. 2023. PMID: 37723892 Free PMC article.
-
Functional Outcomes and Shoulder Instability in Reconstruction of Proximal Humerus Metastases.Curr Oncol. 2023 Mar 24;30(4):3571-3579. doi: 10.3390/curroncol30040272. Curr Oncol. 2023. PMID: 37185385 Free PMC article.
References
-
- Angelini A, Mavrogenis AF, Trovarelli G, et al. Extra-articular shoulder resections: outcomes of 54 patients. J Shoulder Elbow Surg. 2017;26:e337-e345. - PubMed
-
- Below C. Dahlins Bone Tumors: General Aspects And Data On 11 087 Cases. 5th ed. Lippincott-Raven; 1996.
-
- Enneking WF, Dunham W, Gebhardt MC, Malawar M, Pritchard DJ. A system for the functional evaluation of reconstructive procedures after surgical treatment of tumors of the musculoskeletal system. Clin Orthop Relat Res. 1993;(286):241-246. - PubMed
-
- Gosheger G, Hardes J, Ahrens H, Gebert C, Winkelman W. Endoprosthetic replacement of the humerus combined with trapezius and latissimus dorsi transfer: a report of three patients. Arch Orthop Trauma Surg. 2005;125:62-65. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
