

Evaluation of Optimal Diastolic Blood Pressure Range Among Adults With Treated Systolic Blood Pressure Less Than 130 mm Hg
- PMID: 33595663
- PMCID: PMC7890449
- DOI: 10.1001/jamanetworkopen.2020.37554
Evaluation of Optimal Diastolic Blood Pressure Range Among Adults With Treated Systolic Blood Pressure Less Than 130 mm Hg
Abstract
Importance: Extremely low diastolic blood pressure has been reported to be associated with increased adverse cardiovascular events (ie, the diastolic J-shape phenomenon); however, current US guidelines recommend an intensive blood pressure target of less than 130/80 mm Hg without mentioning the lower limits of diastolic blood pressure.
Objectives: To evaluate whether there is a diastolic J-shape phenomenon for patients with an treated systolic blood pressure of less than 130 mm Hg and to explore the safe and optimal diastolic blood pressure ranges for this patient population.
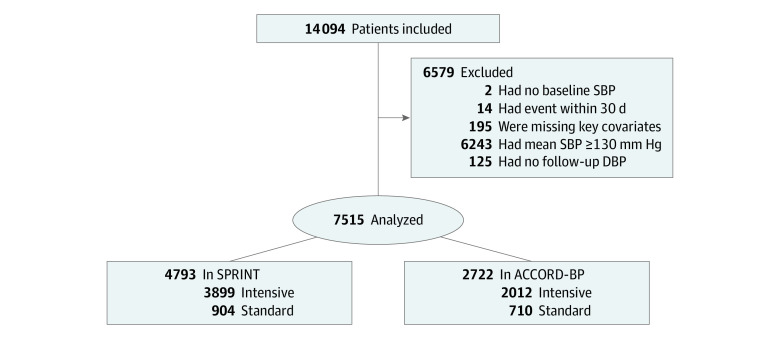
Design, setting, and participants: This cohort study analyzed outcome data of patients at high cardiovascular risk who were randomized to intensive or standard blood pressure control and achieved treated systolic blood pressure of less than 130 mm Hg in the Systolic Blood Pressure Intervention Trial (SPRINT) and Action to Control Cardiovascular Risk in Diabetes-Blood Pressure (ACCORD-BP) trial. Data were collected from October 2010 to August 2015 (SPRINT) and from September 1999 to June 2009 (ACCORD-BP). Data were analyzed from January to May 2020.
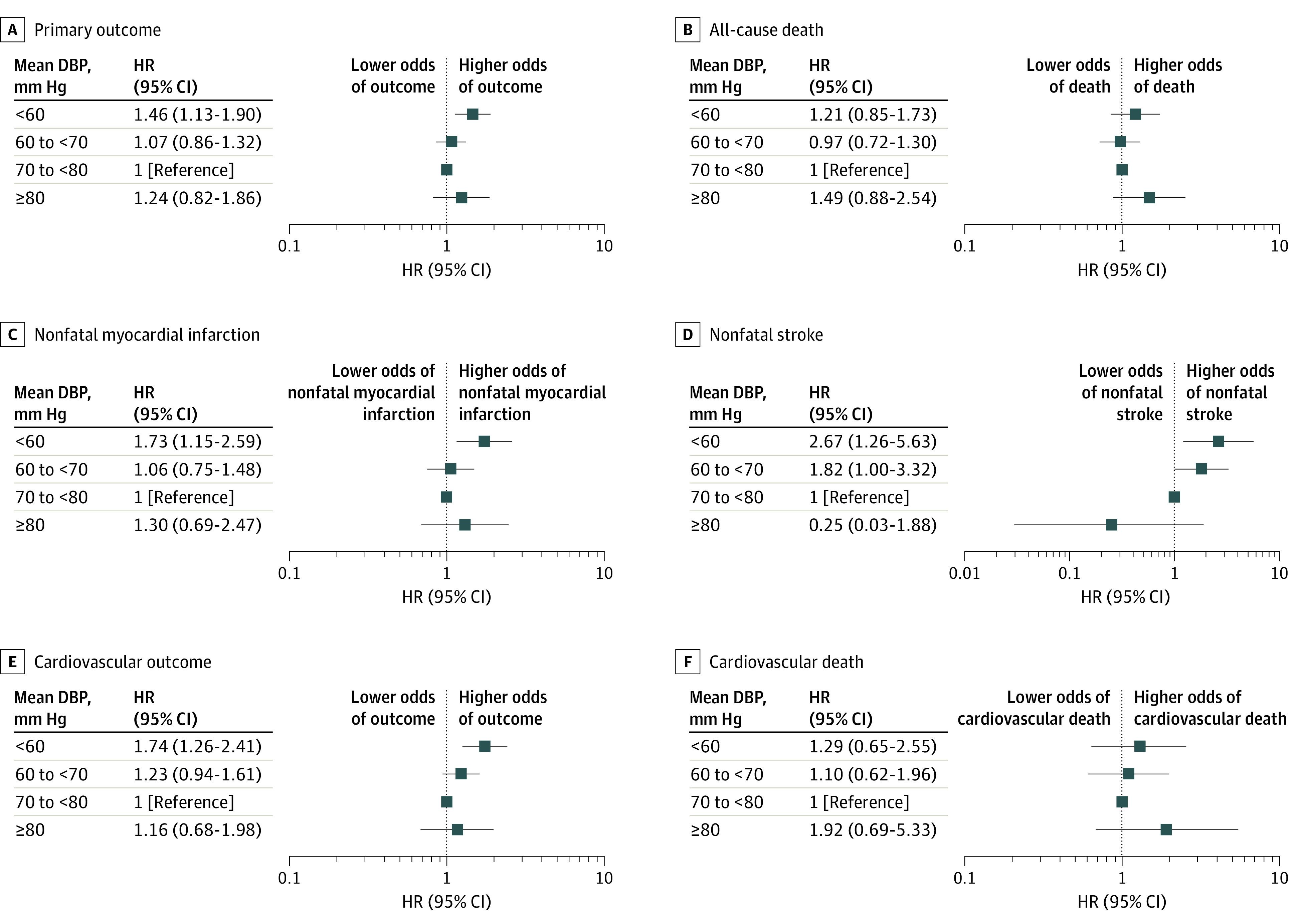
Exposure: Treated diastolic blood pressure, divided in intervals of less than 60, 60 to less than 70, 70 to less than 80, and 80 mm Hg and greater.
Main outcomes and measures: The primary outcome was a composite of all-cause death, nonfatal myocardial infarction, and nonfatal stroke. A composite cardiovascular outcome, including cardiovascular death, nonfatal myocardial infarction, and nonfatal stroke, was among the key secondary outcomes.
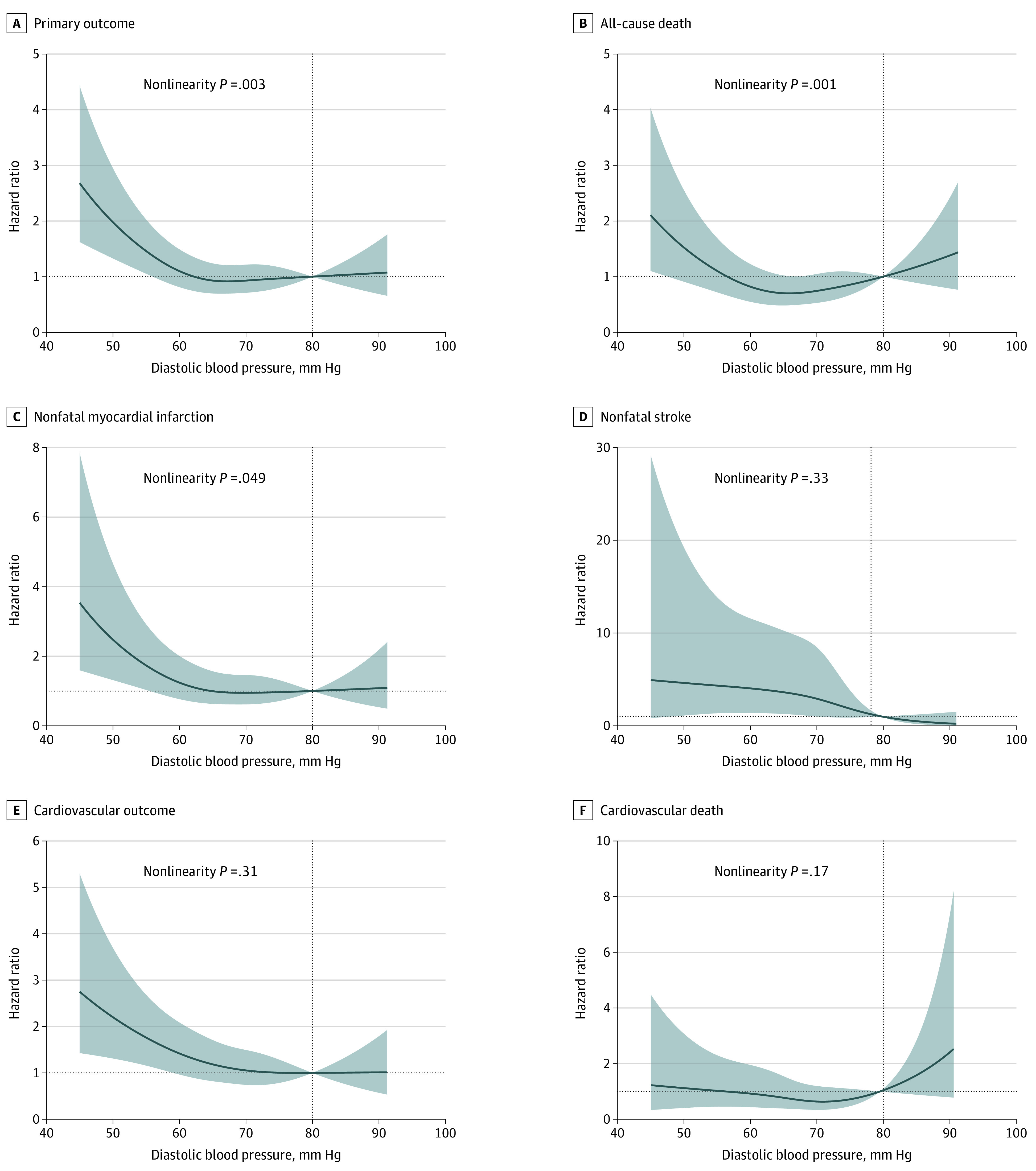
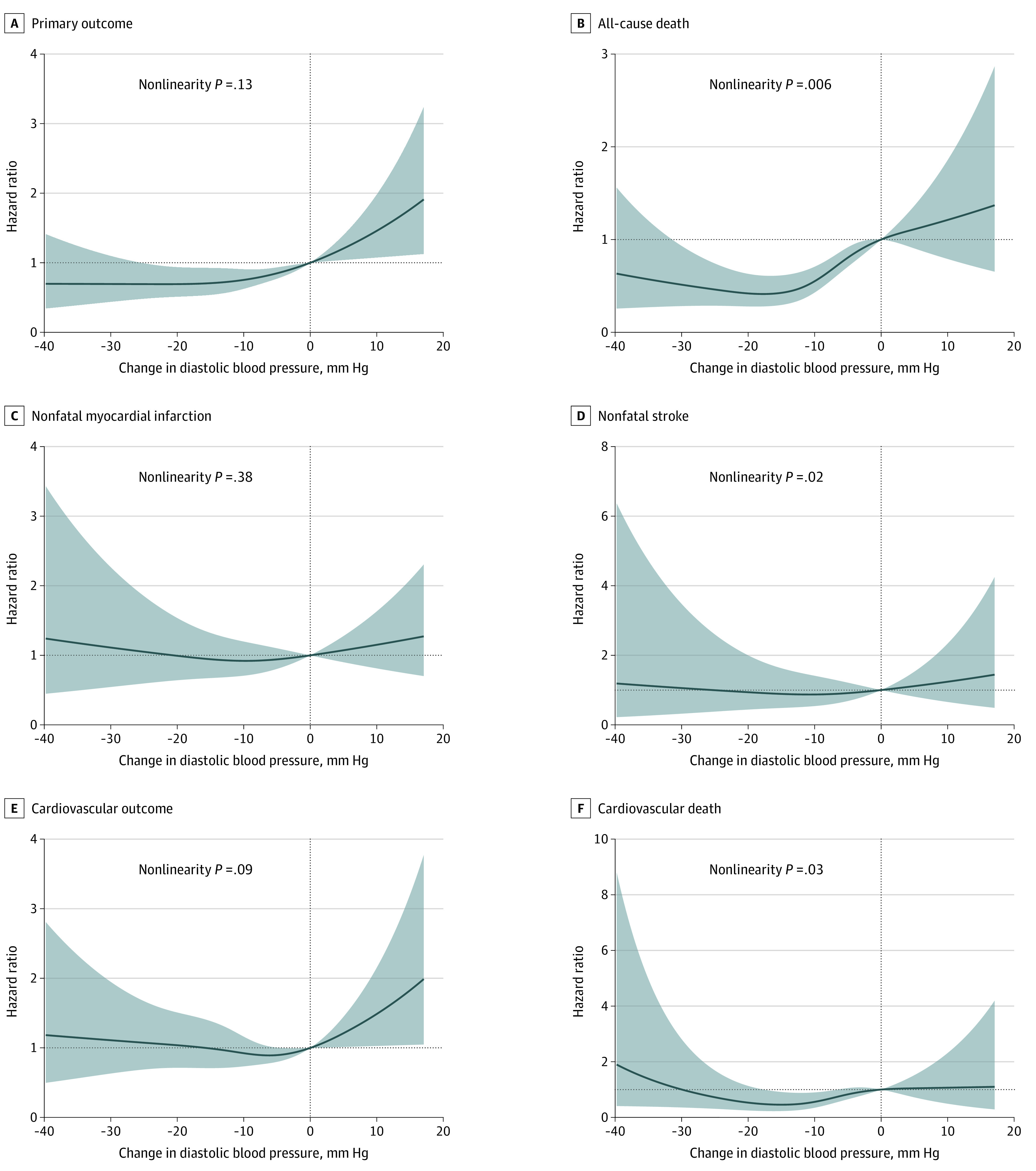
Results: A total of 7515 patients (mean [SD] age, 65.6 [8.7] years; 4553 [60.6%] men) were included in this analysis. The nominally lowest risk was observed at a diastolic blood pressure between 70 and 80 mm Hg for the primary outcome, the composite cardiovascular outcome, nonfatal myocardial infarction, and cardiovascular death. A mean diastolic blood pressure of less than 60 mm Hg was associated with significantly increased risk of the primary outcome (hazard ratio [HR], 1.46; 95% CI, 1.13-1.90; P = .004), the composite cardiovascular outcome (HR, 1.74; 95% CI, 1.26-2.41; P = .001), nonfatal myocardial infarction (HR, 1.73; 95% CI, 1.15-2.59; P = .008), and nonfatal stroke (HR, 2.67; 95% CI, 1.26-5.63; P = .01).
Conclusions and relevance: This cohort study found that lowering diastolic blood pressure to less than 60 mm Hg was associated with increased risk of cardiovascular events in patients with high cardiovascular risk and an treated systolic blood pressure less than 130 mm Hg. The finding that a diastolic blood pressure value between 70 and 80 mm Hg was an optimum target for this patient population merits further study.
Conflict of interest statement
Figures
Similar articles
-
Association Between Baseline Diastolic Blood Pressure and the Efficacy of Intensive vs Standard Blood Pressure-Lowering Therapy.JAMA Netw Open. 2021 Oct 1;4(10):e2128980. doi: 10.1001/jamanetworkopen.2021.28980. JAMA Netw Open. 2021. PMID: 34668944 Free PMC article.
-
Intensive vs Standard Blood Pressure Control and Cardiovascular Disease Outcomes in Adults Aged ≥75 Years: A Randomized Clinical Trial.JAMA. 2016 Jun 28;315(24):2673-82. doi: 10.1001/jama.2016.7050. JAMA. 2016. PMID: 27195814 Free PMC article. Clinical Trial.
-
[The SPRINT Research. A Randomized Trial of Intensive versus Standard Blood-Pressure Control].Vnitr Lek. 2016 Jan;62(1):44-7. Vnitr Lek. 2016. PMID: 26967236 Clinical Trial. Czech.
-
Blood pressure targets in adults with hypertension.Cochrane Database Syst Rev. 2020 Dec 17;12(12):CD004349. doi: 10.1002/14651858.CD004349.pub3. Cochrane Database Syst Rev. 2020. PMID: 33332584 Free PMC article.
-
Blood pressure targets for the treatment of people with hypertension and cardiovascular disease.Cochrane Database Syst Rev. 2020 Sep 9;9(9):CD010315. doi: 10.1002/14651858.CD010315.pub4. Cochrane Database Syst Rev. 2020. Update in: Cochrane Database Syst Rev. 2022 Nov 18;11:CD010315. doi: 10.1002/14651858.CD010315.pub5. PMID: 32905623 Free PMC article. Updated.
Cited by
-
Low Diastolic Blood Pressure and Mortality in Older Women. Results From the Women's Health Initiative Long Life Study.Am J Hypertens. 2022 Sep 1;35(9):795-802. doi: 10.1093/ajh/hpac056. Am J Hypertens. 2022. PMID: 35522983 Free PMC article.
-
Impact of baseline blood pressure on adverse outcomes in Japanese patients with non-valvular atrial fibrillation: the J-RISK AF.Eur Heart J Open. 2022 Dec 16;2(6):oeac081. doi: 10.1093/ehjopen/oeac081. eCollection 2022 Nov. Eur Heart J Open. 2022. PMID: 36583077 Free PMC article.
-
The Diastolic Blood Pressure J-Curve in Hypertension Management: Links and Risk for Cardiovascular Disease.Integr Blood Press Control. 2021 Dec 14;14:179-187. doi: 10.2147/IBPC.S286957. eCollection 2021. Integr Blood Press Control. 2021. PMID: 34938115 Free PMC article. Review.
-
Ten-year risk assessment for cardiovascular diseases using ASCVD risk estimator plus: outcomes from hypertension and diabetes patients.Diabetol Metab Syndr. 2023 Oct 27;15(1):216. doi: 10.1186/s13098-023-01170-2. Diabetol Metab Syndr. 2023. PMID: 37891666 Free PMC article.
-
Impact of Frailty on the Relationship between Blood Pressure and Cardiovascular Diseases and Mortality in Young-Old Adults.J Pers Med. 2022 Mar 8;12(3):418. doi: 10.3390/jpm12030418. J Pers Med. 2022. PMID: 35330418 Free PMC article.
References
-
- Lewington S, Clarke R, Qizilbash N, Peto R, Collins R; Prospective Studies Collaboration . Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet. 2002;360(9349):1903-1913. doi:10.1016/S0140-6736(02)11911-8 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
