

Prone Positioning and Survival in Mechanically Ventilated Patients With Coronavirus Disease 2019-Related Respiratory Failure
- PMID: 33595960
- PMCID: PMC8277560
- DOI: 10.1097/CCM.0000000000004938
Prone Positioning and Survival in Mechanically Ventilated Patients With Coronavirus Disease 2019-Related Respiratory Failure
Abstract
Objectives: Therapies for patients with respiratory failure from coronavirus disease 2019 are urgently needed. Early implementation of prone positioning ventilation improves survival in patients with acute respiratory distress syndrome, but studies examining the effect of proning on survival in patients with coronavirus disease 2019 are lacking. Our objective was to estimate the effect of early proning initiation on survival in patients with coronavirus disease 2019-associated respiratory failure.
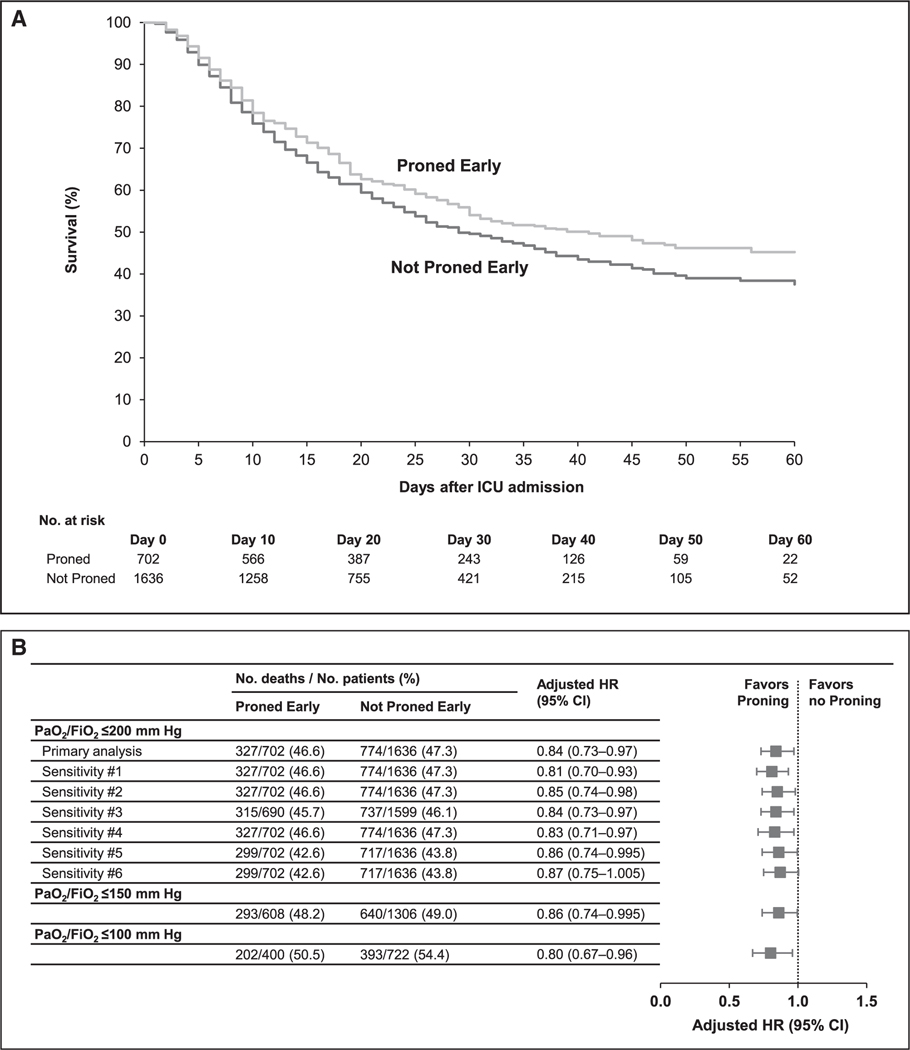
Design: Data were derived from the Study of the Treatment and Outcomes in Critically Ill Patients with coronavirus disease 2019, a multicenter cohort study of critically ill adults with coronavirus disease 2019 admitted to 68 U.S. hospitals. Using these data, we emulated a target trial of prone positioning ventilation by categorizing mechanically ventilated hypoxemic (ratio of Pao2 over the corresponding Fio2 ≤ 200 mm Hg) patients as having been initiated on proning or not within 2 days of ICU admission. We fit an inverse probability-weighted Cox model to estimate the mortality hazard ratio for early proning versus no early proning. Patients were followed until death, hospital discharge, or end of follow-up.
Setting: ICUs at 68 U.S. sites.
Patients: Critically ill adults with laboratory-confirmed coronavirus disease 2019 receiving invasive mechanical ventilation with ratio of Pao2 over the corresponding Fio2 less than or equal to 200 mm Hg.
Interventions: None.
Measurements and main results: Among 2,338 eligible patients, 702 (30.0%) were proned within the first 2 days of ICU admission. After inverse probability weighting, baseline and severity of illness characteristics were well-balanced between groups. A total of 1,017 (43.5%) of the 2,338 patients were discharged alive, 1,101 (47.1%) died, and 220 (9.4%) were still hospitalized at last follow-up. Patients proned within the first 2 days of ICU admission had a lower adjusted risk of death compared with nonproned patients (hazard ratio, 0.84; 95% CI, 0.73-0.97).
Conclusions: In-hospital mortality was lower in mechanically ventilated hypoxemic patients with coronavirus disease 2019 treated with early proning compared with patients whose treatment did not include early proning.
Copyright © 2021 by the Society of Critical Care Medicine and Wolters Kluwer Health, Inc. All Rights Reserved.
Conflict of interest statement
Dr. Mathews reported receiving grants from the National Institute of Health (NIH) and the National Heart, Lung, and Blood Institute (NHLBI) during the conduct of the study and serves on the steering committee for A Multi-Center, Adaptive, Randomized, Double-blind, Placebo-controlled Study to Assess the Efficacy and Safety of Gimsilumab in Subjects With Lung Injury or Acute Respiratory Distress Syndrome Secondary to COVID-19 (BREATHE) trial, funded by Roivant/Kinevant Sciences; she received support for article research from NIH. Dr. Shaefi reported receiving grants from the NIH and the National Institute on Aging and the National Institute of General Medical Sciences; he received support for article research from NIH. Dr. Coca received funding from RenalytixAI, Relypsa, Takeda Pharmaceuticals, CHF Solutions, Bayer, Boehringer Ingelheim, Akebia, inRegen, Renal Research Institute, and XORTX Therapeutics, Inc.; he owns equities in RenalytixAI and pulseData. Dr. Gupta reported receiving grants from the NIH and is a scientific coordinator for GlaxoSmithKline’s Anemia Studies in Chronic Kidney Disease: Erythropoiesis via a Novel Prolyl Hydroxylase Inhibitor Daprodustat trial. Dr. Srivastava’s institution received funding from the NIH and National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK); he reported receiving funding from the NIH, NIDDK, Horizon Therapeutics PLC, AstraZeneca, Tate & Latham, and CVS Caremark. Dr. Hernán reported receiving grants from the NIH. Dr. Chan’s institution received funding from NIH and Renal Research Institute; she received funding from Gerson Lehrman Group consulting and NIH; she received support for article research from NIH. Dr. Leaf’s institution received funding from NIH, NIDDK, and NHLBI; he received funding from BioPorto. The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures


Comment in
-
Prone Positioning in Coronavirus Disease 2019: Just Do It!Crit Care Med. 2021 Jul 1;49(7):1186-1188. doi: 10.1097/CCM.0000000000004979. Crit Care Med. 2021. PMID: 34135274 No abstract available.
References
-
- Centers for Disease Control and Prevention: Coronavirus Disease 2019 (COVID-19), Cases, Data & Surveillance, 2020. Available at: https://www.cdc.gov/coronavirus/2019-ncov/cases-updates/cases-in-us.html. Accessed December 6, 2020
-
- Lim WS, Emberson JR, Mafham M, et al. ; The RECOVERY Collaborative Group: Dexamethasone in hospitalized patients with COVID-19 — preliminary report. N Engl J Med 2020. Jul 17. [online ahead of print]
-
- Guérin C, Reignier J, Richard JC, et al. ; PROSEVA Study Group: Prone positioning in severe acute respiratory distress syndrome. N Engl J Med 2013; 368:2159–2168 - PubMed
-
- Fan E, Del Sorbo L, Goligher EC, et al. ; American Thoracic Society, European Society of Intensive Care Medicine, and Society of Critical Care Medicine: An official American thoracic society/European society of intensive care medicine/society of critical care medicine clinical practice guideline: Mechanical ventilation in adult patients with acute respiratory distress syndrome. Am J Respir Crit Care Med 2017; 195:1253–1263 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
