

Treatment of Uterine Fibroid Symptoms with Relugolix Combination Therapy
- PMID: 33596357
- PMCID: PMC8262231
- DOI: 10.1056/NEJMoa2008283
Treatment of Uterine Fibroid Symptoms with Relugolix Combination Therapy
Abstract
Background: Uterine fibroids are a common cause of heavy menstrual bleeding and pain. Treatment with the combination of relugolix (an oral gonadotropin-releasing hormone-receptor antagonist), estradiol, and norethindrone acetate, administered once daily, may have efficacy in women with uterine fibroids and heavy bleeding while avoiding hypoestrogenic effects.
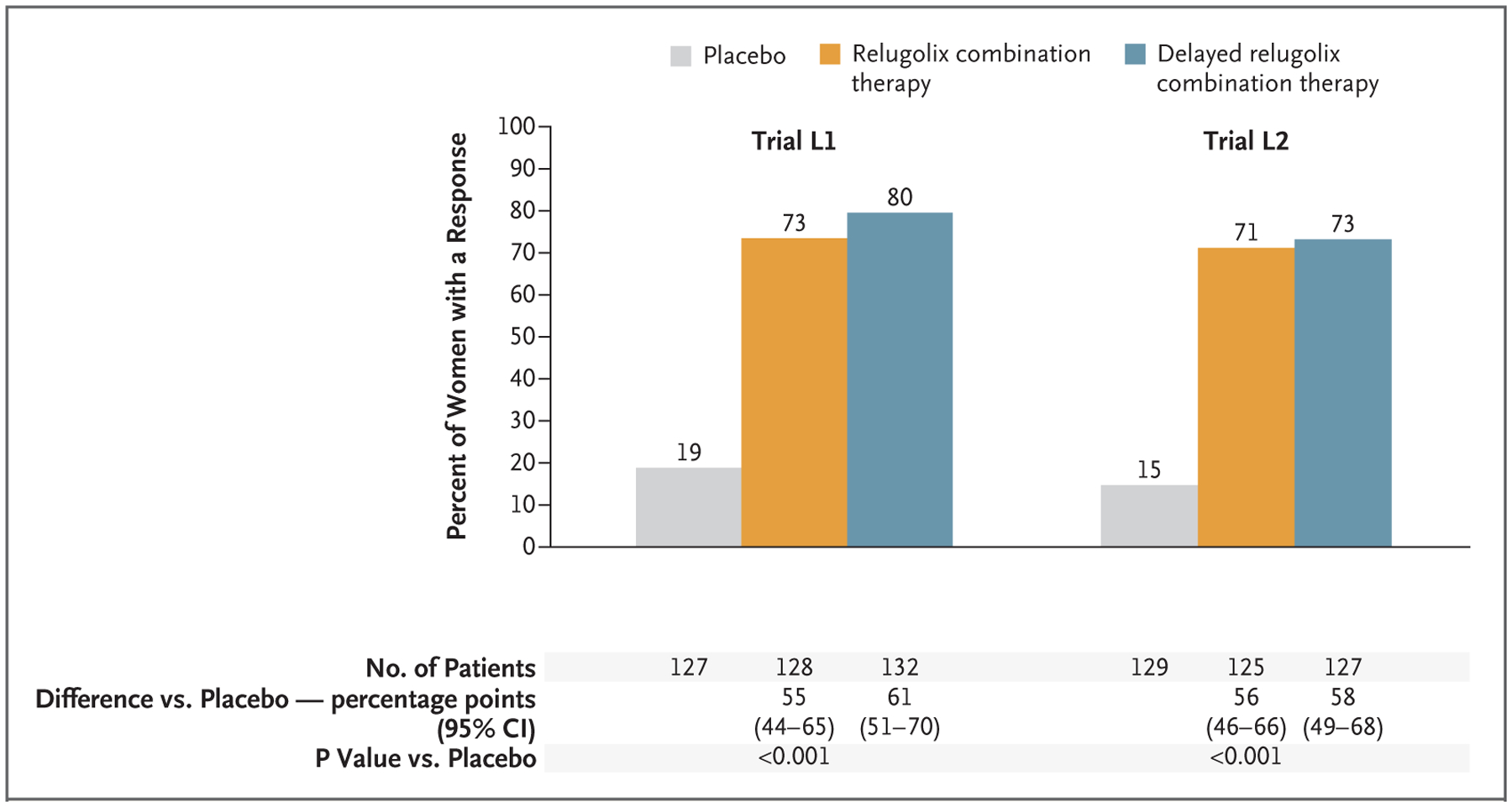
Methods: We conducted two replicate international, double-blind, 24-week, phase 3 trials involving women with fibroid-associated heavy menstrual bleeding. Participants were randomly assigned in a 1:1:1 ratio to receive once-daily placebo, relugolix combination therapy (40 mg of relugolix, 1 mg of estradiol, and 0.5 mg of norethindrone acetate), or delayed relugolix combination therapy (40 mg of relugolix monotherapy, followed by relugolix combination therapy, each for 12 weeks). The primary efficacy end point in each trial was the percentage of participants with a response (volume of menstrual blood loss <80 ml and a ≥50% reduction in volume from baseline) in the relugolix combination therapy group, as compared with the placebo group. Key secondary end points were amenorrhea, volume of menstrual blood loss, distress from bleeding and pelvic discomfort, anemia, pain, fibroid volume, and uterine volume. Safety and bone mineral density were assessed.
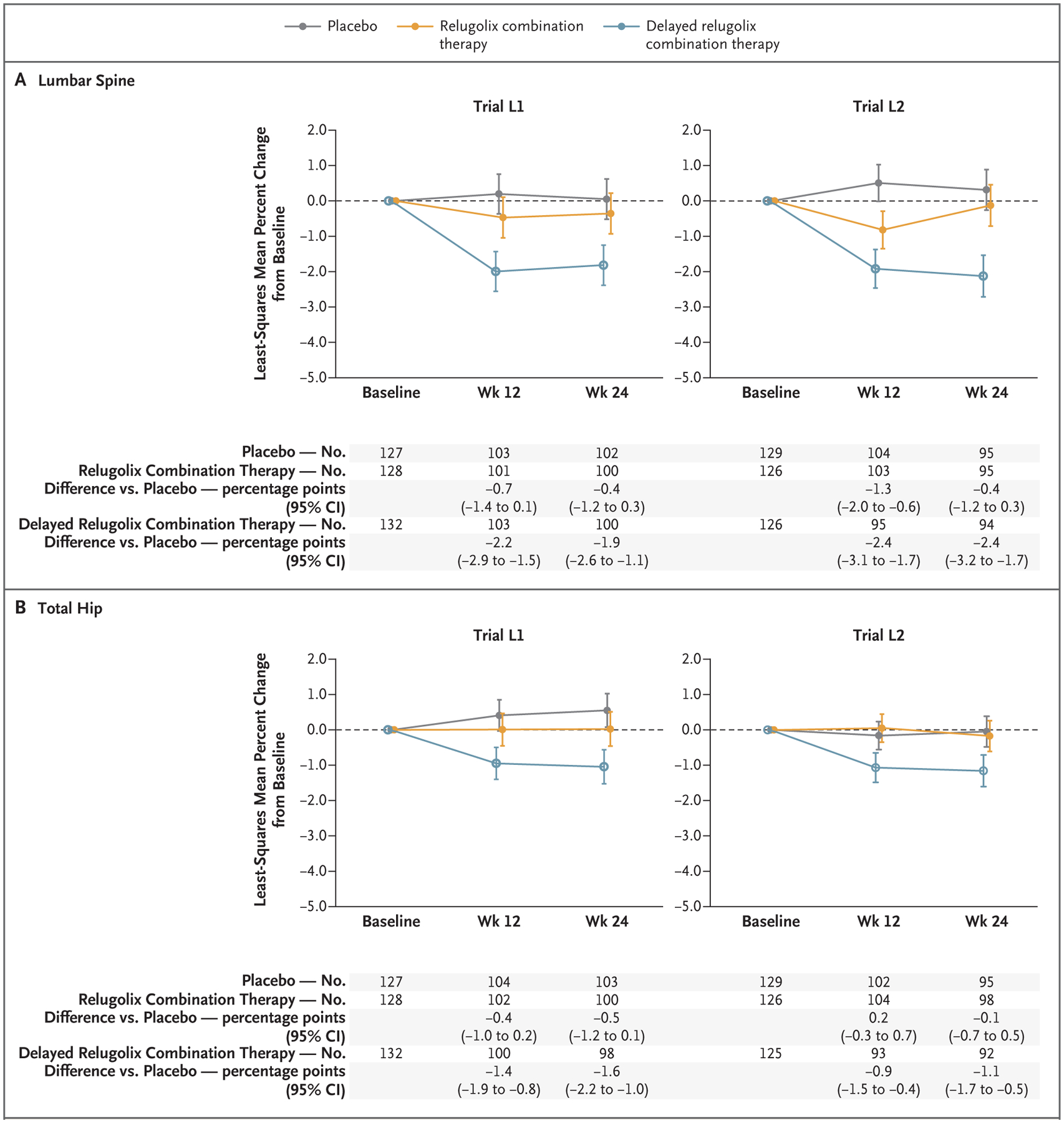
Results: A total of 388 women in trial L1 and 382 in trial L2 underwent randomization. A total of 73% of the participants in the relugolix combination therapy group in trial L1 and 71% of those in trial L2 had a response (primary end point), as compared with 19% and 15%, respectively, of those in the placebo groups (P<0.001 for both comparisons). Both relugolix combination therapy groups had significant improvements, as compared with the placebo groups, in six of seven key secondary end points, including measures of menstrual blood loss (including amenorrhea), pain, distress from bleeding and pelvic discomfort, anemia, and uterine volume, but not fibroid volume. The incidence of adverse events was similar with relugolix combination therapy and placebo. Bone mineral density was similar with relugolix combination therapy and placebo but decreased with relugolix monotherapy.
Conclusions: Once-daily relugolix combination therapy resulted in a significant reduction in menstrual bleeding, as compared with placebo, and preserved bone mineral density in women with uterine fibroids. (Funded by Myovant Sciences; LIBERTY 1 [L1] and LIBERTY 2 [L2] ClinicalTrials.gov numbers, NCT03049735 and NCT03103087, respectively.).
Copyright © 2021 Massachusetts Medical Society.
Figures
Comment in
-
Relugolix - new treatment for uterine fibroid-related heavy bleeding.Nat Rev Endocrinol. 2021 Jun;17(6):321-322. doi: 10.1038/s41574-021-00493-2. Nat Rev Endocrinol. 2021. PMID: 33854216 No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical