

Patterns of myocardial injury in recovered troponin-positive COVID-19 patients assessed by cardiovascular magnetic resonance
- PMID: 33596594
- PMCID: PMC7928984
- DOI: 10.1093/eurheartj/ehab075
Patterns of myocardial injury in recovered troponin-positive COVID-19 patients assessed by cardiovascular magnetic resonance
Abstract
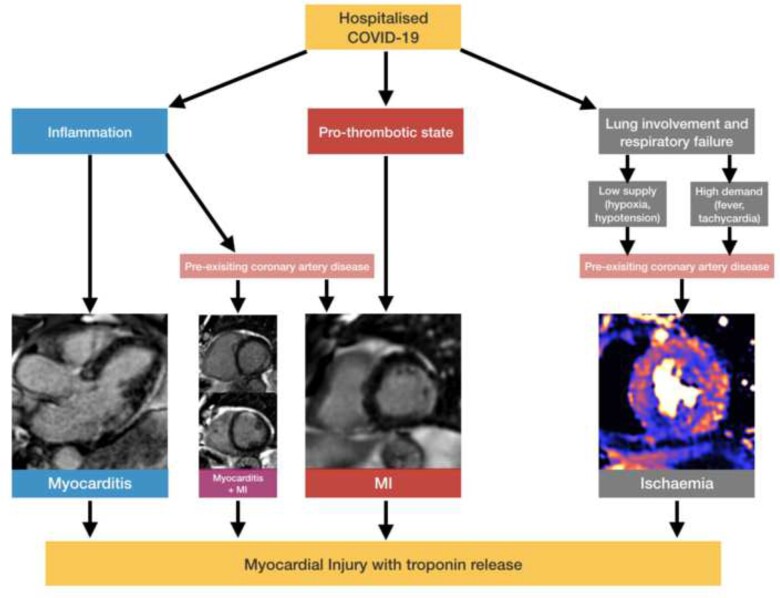
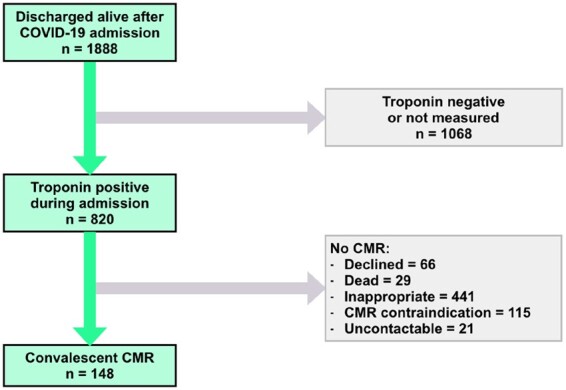
Background: Troponin elevation is common in hospitalized COVID-19 patients, but underlying aetiologies are ill-defined. We used multi-parametric cardiovascular magnetic resonance (CMR) to assess myocardial injury in recovered COVID-19 patients.
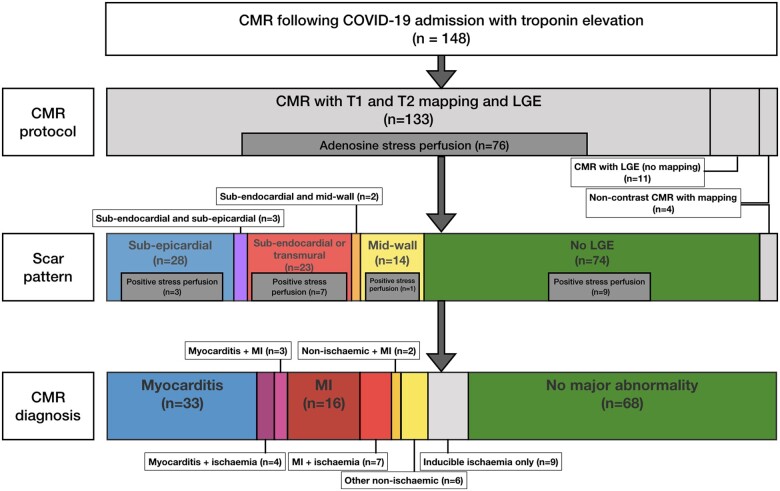
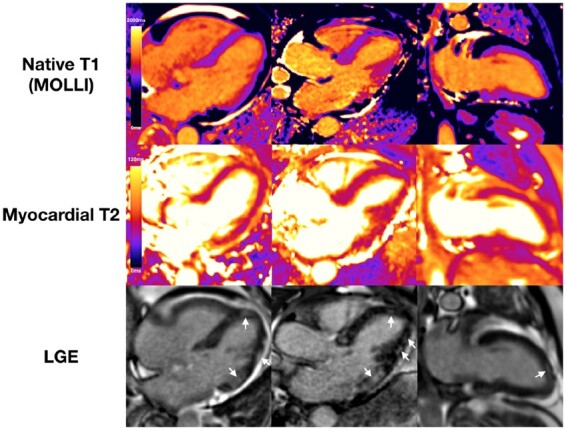
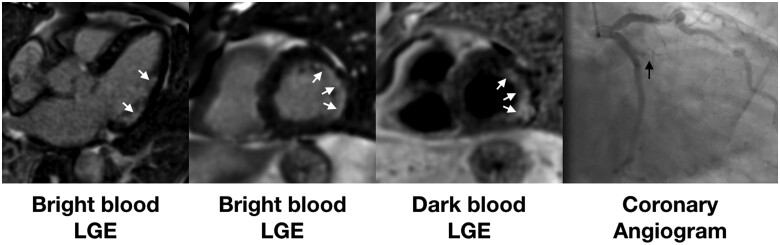
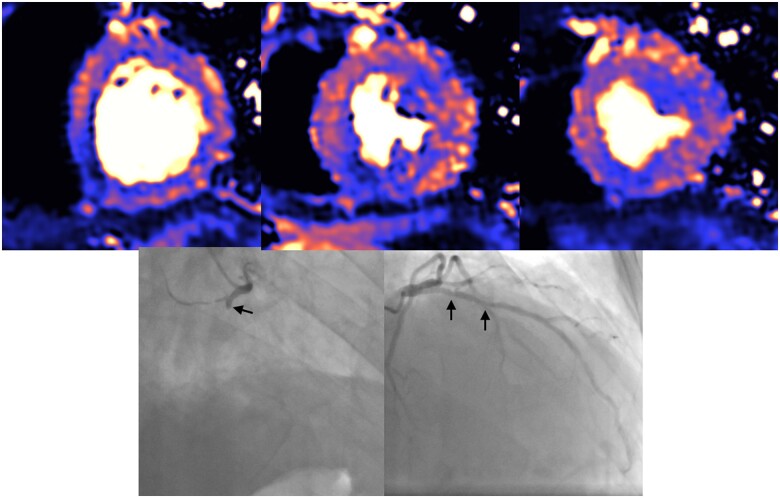
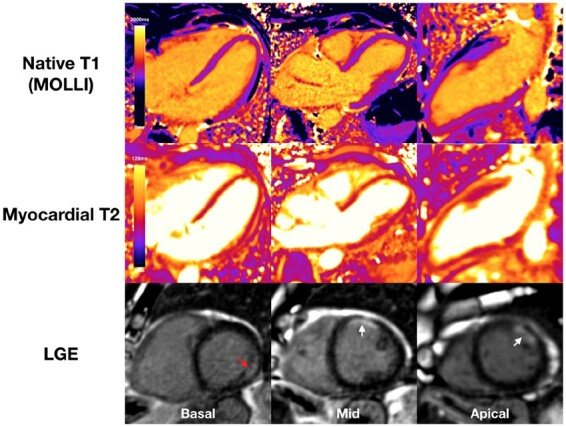
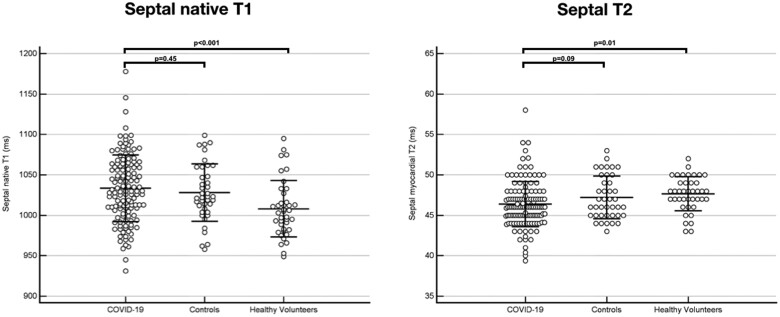
Methods and results: One hundred and forty-eight patients (64 ± 12 years, 70% male) with severe COVID-19 infection [all requiring hospital admission, 48 (32%) requiring ventilatory support] and troponin elevation discharged from six hospitals underwent convalescent CMR (including adenosine stress perfusion if indicated) at median 68 days. Left ventricular (LV) function was normal in 89% (ejection fraction 67% ± 11%). Late gadolinium enhancement and/or ischaemia was found in 54% (80/148). This comprised myocarditis-like scar in 26% (39/148), infarction and/or ischaemia in 22% (32/148) and dual pathology in 6% (9/148). Myocarditis-like injury was limited to three or less myocardial segments in 88% (35/40) of cases with no associated LV dysfunction; of these, 30% had active myocarditis. Myocardial infarction was found in 19% (28/148) and inducible ischaemia in 26% (20/76) of those undergoing stress perfusion (including 7 with both infarction and ischaemia). Of patients with ischaemic injury pattern, 66% (27/41) had no past history of coronary disease. There was no evidence of diffuse fibrosis or oedema in the remote myocardium (T1: COVID-19 patients 1033 ± 41 ms vs. matched controls 1028 ± 35 ms; T2: COVID-19 46 ± 3 ms vs. matched controls 47 ± 3 ms).
Conclusions: During convalescence after severe COVID-19 infection with troponin elevation, myocarditis-like injury can be encountered, with limited extent and minimal functional consequence. In a proportion of patients, there is evidence of possible ongoing localized inflammation. A quarter of patients had ischaemic heart disease, of which two-thirds had no previous history. Whether these observed findings represent pre-existing clinically silent disease or de novo COVID-19-related changes remain undetermined. Diffuse oedema or fibrosis was not detected.
Keywords: COVID-19; Cardiovascular magnetic resonance; Myocardial infarction; Myocardial oedema; Myocarditis; SARS-CoV-2.
© The Author(s) 2021. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
Comment in
-
What we (don't) know about myocardial injury after COVID-19.Eur Heart J. 2021 May 14;42(19):1879-1882. doi: 10.1093/eurheartj/ehab145. Eur Heart J. 2021. PMID: 33713116 Free PMC article. No abstract available.
-
The Janus of COVID-19: from registry data to prospective studies.Eur Heart J. 2021 Aug 7;42(30):2951-2952. doi: 10.1093/eurheartj/ehab238. Eur Heart J. 2021. PMID: 34166487 Free PMC article. No abstract available.
-
The evolution of cardiovascular COVID-19 research.Eur Heart J. 2021 Aug 7;42(30):2953-2954. doi: 10.1093/eurheartj/ehab240. Eur Heart J. 2021. PMID: 34166510 Free PMC article. No abstract available.
References
-
- Liu PP, Blet A, Smyth D, Li H. The science underlying COVID-19: implications for the cardiovascular system. Circulation 2020;142:68–78. - PubMed
-
- Moore JB, June CH. Cytokine release syndrome in severe COVID-19. Science 2020;368:473–474. - PubMed
-
- Long B, Long DA, Tannenbaum L, Koyfman A. An emergency medicine approach to troponin elevation due to causes other than occlusion myocardial infarction. Am J Emerg Med 2019;38:998–1006. - PubMed
-
- Vestjens SMT, Spoorenberg SMC, Rijkers GT, Grutters JC, Ten Berg JM, Noordzij PG, Van de Garde EMW, Bos WJW, the Ovidius Study Group. High-sensitivity cardiac troponin T predicts mortality after hospitalization for community-acquired pneumonia. Respirology 2017;22:1000–1006. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
