

Dynamic Detection of Delayed Cerebral Ischemia: A Study in 3 Centers
- PMID: 33596676
- PMCID: PMC8247633
- DOI: 10.1161/STROKEAHA.120.032546
Dynamic Detection of Delayed Cerebral Ischemia: A Study in 3 Centers
Abstract
Background and purpose: Delayed cerebral ischemia (DCI) after aneurysmal subarachnoid hemorrhage negatively impacts long-term recovery but is often detected too late to prevent damage. We aim to develop hourly risk scores using routinely collected clinical data to detect DCI.
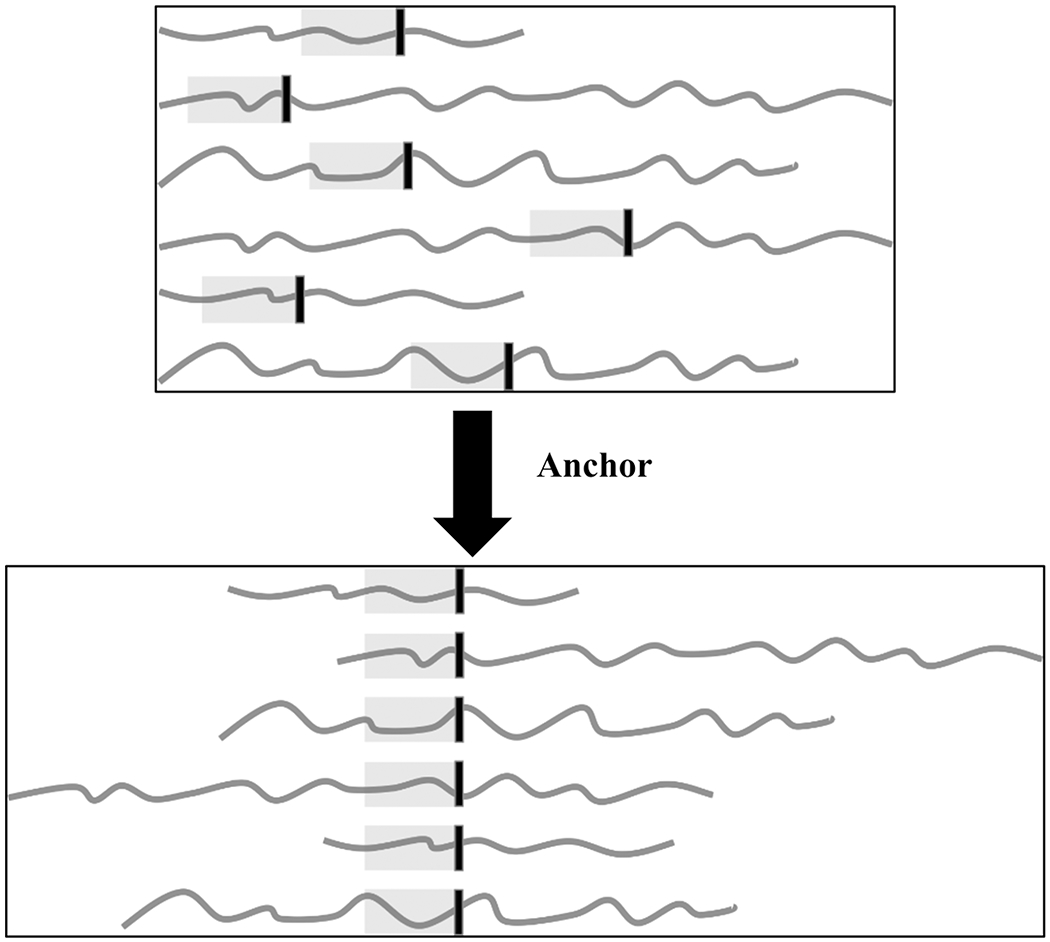
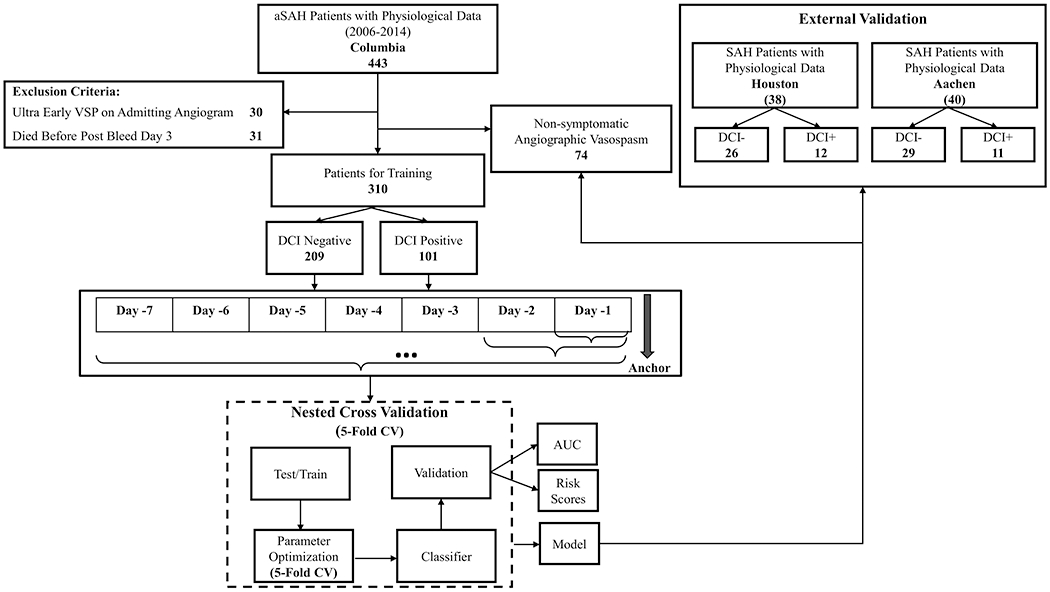
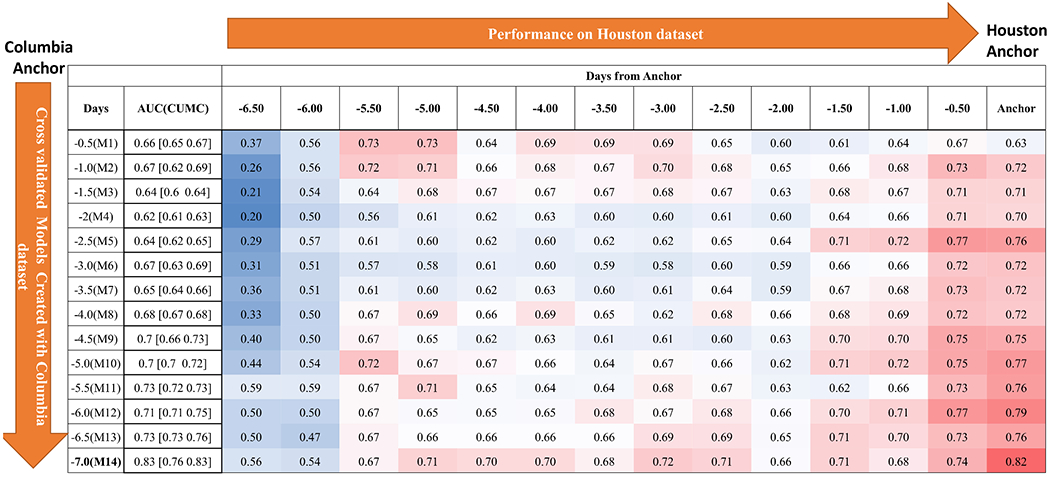
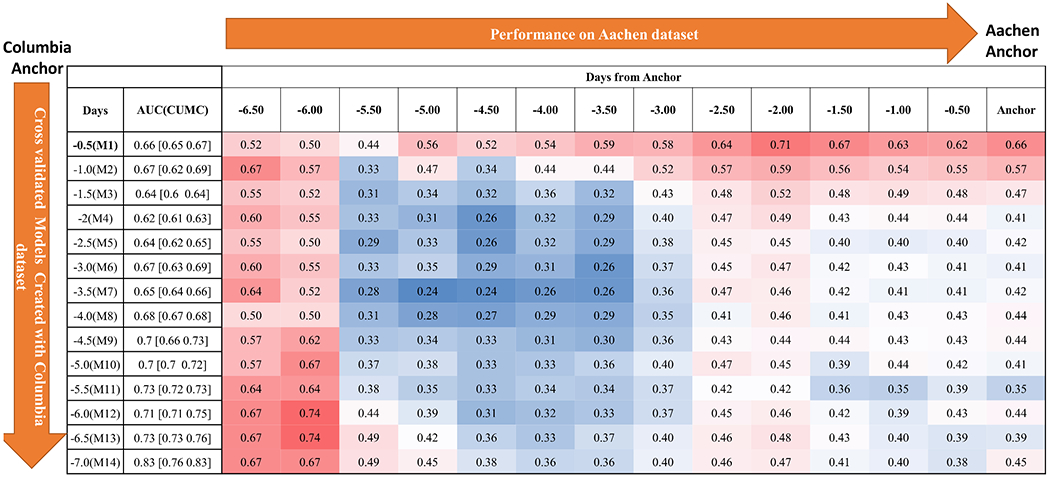
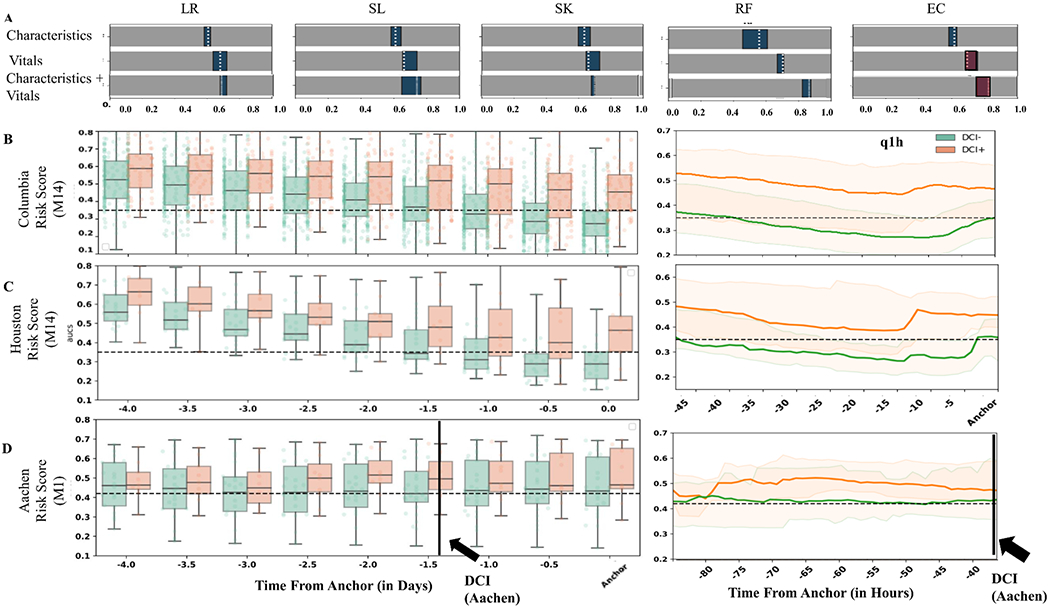
Methods: A DCI classification model was trained using vital sign measurements (heart rate, blood pressure, respiratory rate, and oxygen saturation) and demographics routinely collected for clinical care. Twenty-two time-varying physiological measures were computed including mean, SD, and cross-correlation of heart rate time series with each of the other vitals. Classification was achieved using an ensemble approach with L2-regularized logistic regression, random forest, and support vector machines models. Classifier performance was determined by area under the receiver operating characteristic curves and confusion matrices. Hourly DCI risk scores were generated as the posterior probability at time t using the Ensemble classifier on cohorts recruited at 2 external institutions (n=38 and 40).
Results: Three hundred ten patients were included in the training model (median, 54 years old [interquartile range, 45-65]; 80.2% women, 28.4% Hunt and Hess scale 4-5, 38.7% Modified Fisher Scale 3-4); 101 (33%) developed DCI with a median onset day 6 (interquartile range, 5-8). Classification accuracy before DCI onset was 0.83 (interquartile range, 0.76-0.83) area under the receiver operating characteristic curve. Risk scores applied to external institution datasets correctly predicted 64% and 91% of DCI events as early as 12 hours before clinical detection, with 2.7 and 1.6 true alerts for every false alert.
Conclusions: An hourly risk score for DCI derived from routine vital signs may have the potential to alert clinicians to DCI, which could reduce neurological injury.
Keywords: blood pressure; heart rate; machine learning; respiratory rate; subarachnoid hemorrhage.
Conflict of interest statement
Figures
Comment in
-
Hourly risk score could alert clinicians to delayed cerebral ischaemia.Nat Rev Neurol. 2021 Apr;17(4):194. doi: 10.1038/s41582-021-00481-0. Nat Rev Neurol. 2021. PMID: 33750930 No abstract available.
References
-
- Schmidt J, Wartenberg KE, Fernandez A, Claassen J, Rincon F, Ostapkovich ND, Badjatia N, Parra A, Connolly E, Mayer SA. Frequency and clinical impact of asymptomatic cerebral infarction due to vasospasm after subarachnoid hemorrhage. J Neurosurg. 2008;109:1052–9. doi: 10.3171/jns.2008.109.12.1052 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
