

Left ventricular-arterial coupling as a predictor of stroke volume response to norepinephrine in septic shock - a prospective cohort study
- PMID: 33596822
- PMCID: PMC7886849
- DOI: 10.1186/s12871-021-01276-y
Left ventricular-arterial coupling as a predictor of stroke volume response to norepinephrine in septic shock - a prospective cohort study
Abstract
Background: Left ventricular-arterial coupling (VAC), defined as the ratio of arterial elastance (Ea) to left ventricular end-systolic elastance (Ees), is a key determinant of cardiovascular performance. This study aims to evaluate whether left VAC can predict stroke volume (SV) response to norepinephrine (NE) in septic shock patients.
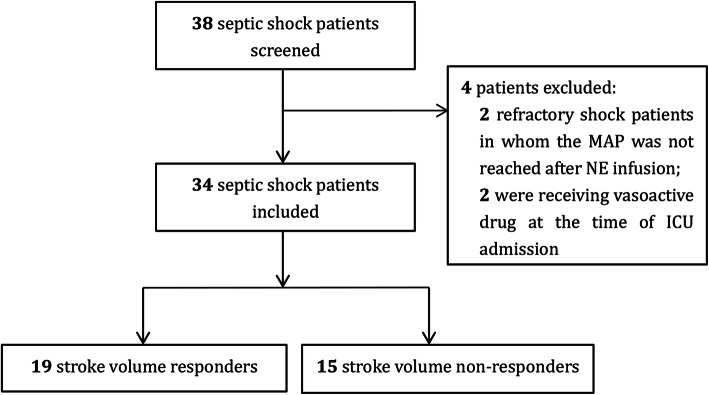
Methods: This was a prospective cohort study conducted in an intensive care unit of a tertiary teaching hospital in China. We recruited septic shock patients who had persistent hypotension despite fluid resuscitation and required NE to maintain mean arterial pressure (MAP) > 65 mmHg. Those patients in whom the target MAP was not reached after NE infusion were ineligible. Echocardiographic variables were measured before (baseline) and after NE infusion. SV responder was defined by a ≥ 15% increase in SV after NE infusion.
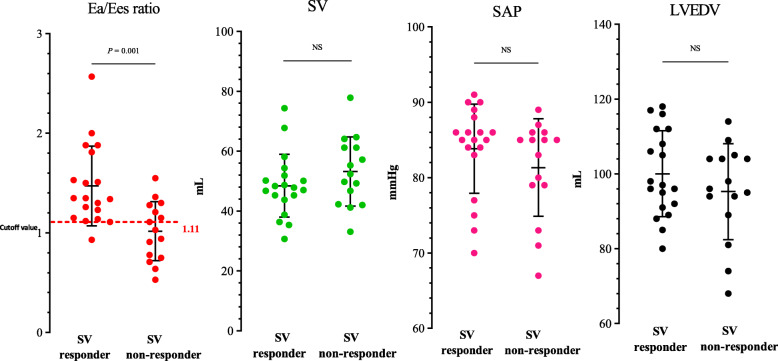
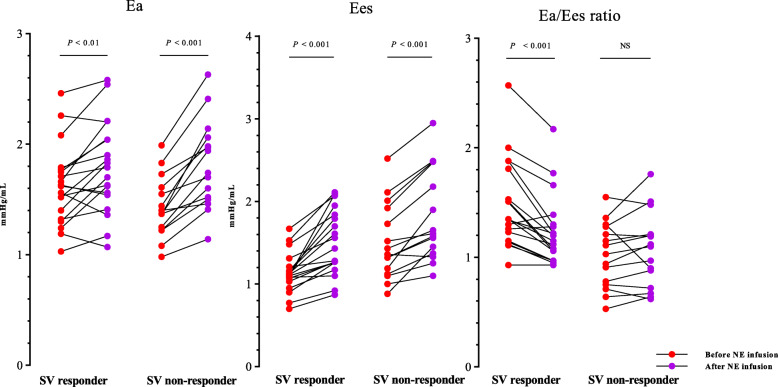
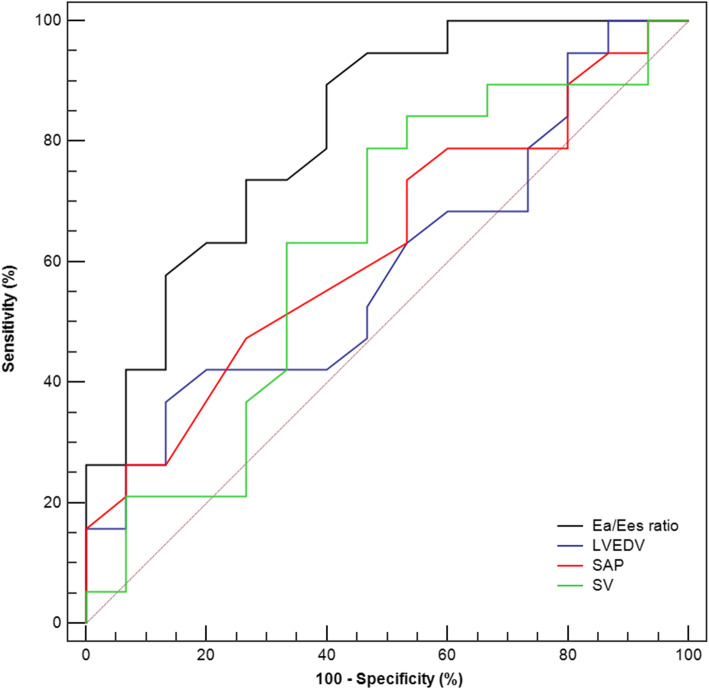
Results: Of 34 septic shock patients included, 19 (56%) were SV responders. Before NE infusion, SV responders had a lower Ees (1.13 ± 0.24 mmHg/mL versus 1.50 ± 0.46 mmHg/mL, P = 0.005) and a higher Ea/Ees ratio (1.47 ± 0.40 versus 1.02 ± 0.30, P = 0.001) than non-responders, and Ea in SV responders was comparable to that in non-responders (1.62 ± 0.36 mmHg/mL versus 1.43 ± 0.28 mmHg/mL, P = 0.092). NE significantly increased Ea and Ees in both groups. The Ea/Ees ratio was normalized by NE administration in SV responders but unchanged in non-responders. The baseline Ea/Ees ratio was positively correlated with NE-induced SV increases (r = 0.688, P < 0.001). Logistic regression analysis indicated that the baseline Ea/Ees ratio was a predictor of SV increases induced by NE (odd ratio 0.008, 95% confidence interval (CI): 0.000 to 0.293), with an area under the receiver operating characteristic curve of 0.816 (95% CI: 0.646 to 0.927).
Conclusions: The left VAC has the ability to predict SV response to NE infusion in septic shock patients.
Trial registration: Chinese Clinical Trial Registry, ChiCTR1900024031, Registered 23 June 2019 - Retrospectively registered, http://www.chictr.org.cn/edit.aspx?pid=40359&htm=4 .
Keywords: Cardiovascular; Norepinephrine; Septic shock; Stroke volume; Ventricular-arterial coupling.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
