

High-sensitive cardiac troponin for the diagnosis of acute myocardial infarction in different chronic kidney disease stages
- PMID: 33596833
- PMCID: PMC7888109
- DOI: 10.1186/s12872-020-01746-0
High-sensitive cardiac troponin for the diagnosis of acute myocardial infarction in different chronic kidney disease stages
Abstract
Background: Chronic kidney disease (CKD) are associated with acute myocardial infarction (AMI). High-sensitive cardiac troponin (hs-cTn) has been evidenced to enhance the early diagnostic accuracy of AMI, but hs-cTn levels are often chronically elevated in CKD patients, which reduces their diagnostic utility. The aim of this study was to derive optimal cutoff-values of hs-cTn levels in patients with CKD and suspected AMI.
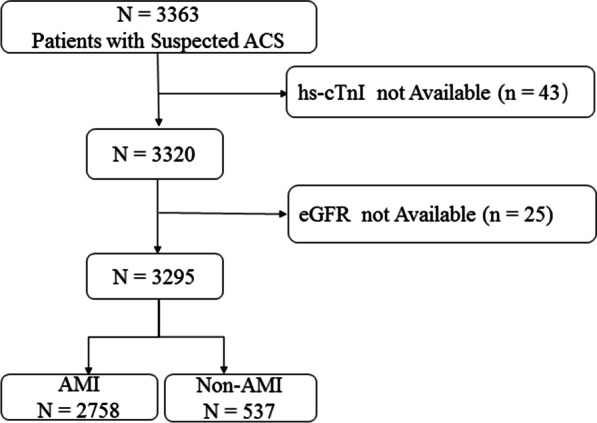
Methods: In this retrospective paper, a total of 3295 patients with chest pain (2758 in AMI group and 537 in Non-AMI group) were recruited, of whom 23.1% were had an estimated glomerular filtration rate (eGFR) of < 60 mL min-1 (1.73 m2)-1. Hs-cTnI values were measured at presentation.
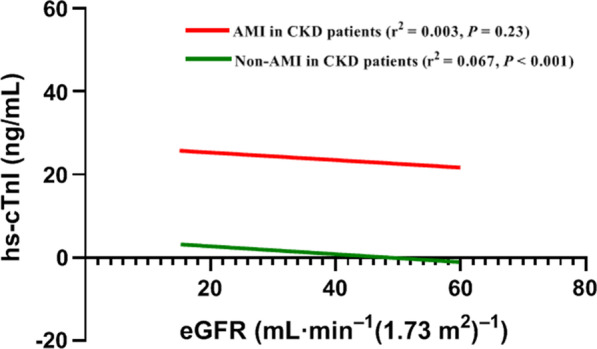
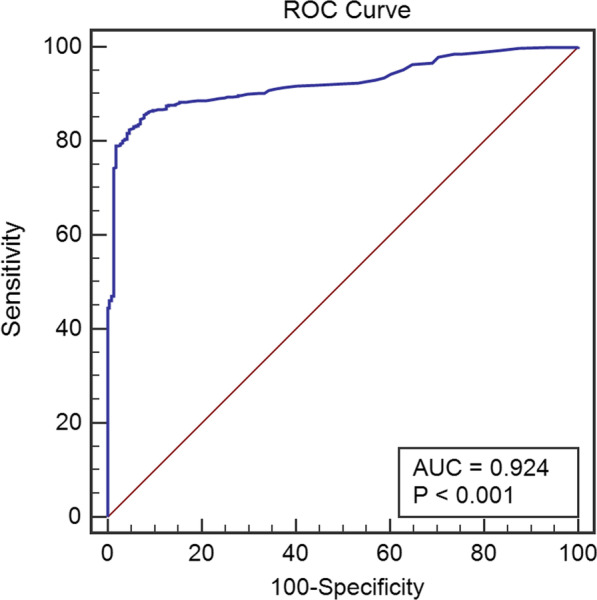
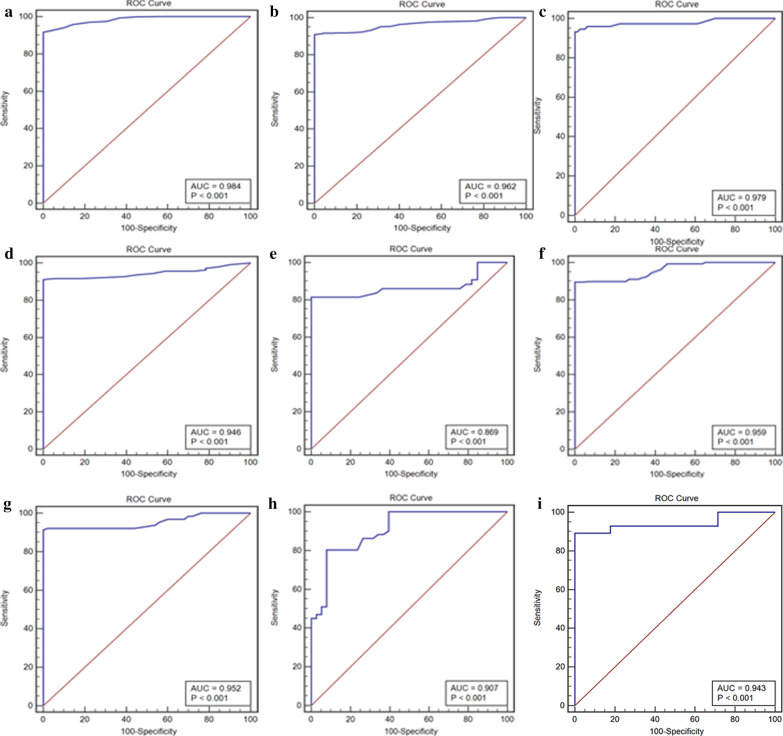
Results: AMI was diagnosed in 83.7% of all patients. The optimal value of hs-TnI in diagnosing AMI was 1.15 ng mL-1, which were higher in males than females comparing different cutoff-values of subgroups divided by age, gender and renal function, and which increased monotonically with decreasing of eGFR because in patients with CKD without AMI, the correlation between hs-cTnI and renal function is low but significant (r2 = 0.067, P < 0.001).
Conclusions: Different optimal cutoff-values of hs-cTnI in the diagnosis of AMI in patients with CKD were helpful to the clinical diagnosis of AMI in various populations and were higher in males than females, but which was needed to be validated by multicenter randomized controlled clinical studies in the future.
Keywords: Acute myocardial infarction; Chronic kidney disease; Estimated glomerular filtration rate; High-sensitivity cardiac troponin.
Conflict of interest statement
Authors stated no conflict of interest
Figures
Similar articles
-
Cardiac Troponins for the Diagnosis of Acute Myocardial Infarction in Chronic Kidney Disease.J Am Heart Assoc. 2018 Oct 2;7(19):e008032. doi: 10.1161/JAHA.117.008032. J Am Heart Assoc. 2018. PMID: 30371308 Free PMC article.
-
Renal Dysfunction Influences the Diagnostic and Prognostic Performance of High-Sensitivity Cardiac Troponin I.J Am Soc Nephrol. 2018 Feb;29(2):636-643. doi: 10.1681/ASN.2017030341. Epub 2017 Oct 27. J Am Soc Nephrol. 2018. PMID: 29079658 Free PMC article.
-
Improving the diagnostic accuracy of acute myocardial infarction with the use of high-sensitive cardiac troponin T in different chronic kidney disease stages.Sci Rep. 2017 Feb 1;7:41350. doi: 10.1038/srep41350. Sci Rep. 2017. PMID: 28145489 Free PMC article.
-
Use and interpretation of high sensitivity cardiac troponins in patients with chronic kidney disease with and without acute myocardial infarction.Clin Biochem. 2015 Mar;48(4-5):247-53. doi: 10.1016/j.clinbiochem.2015.01.004. Epub 2015 Jan 22. Clin Biochem. 2015. PMID: 25617663 Review.
-
High-sensitivity-cardiac troponin for accelerated diagnosis of acute myocardial infarction: A systematic review and meta-analysis.Am J Emerg Med. 2020 Jul;38(7):1402-1407. doi: 10.1016/j.ajem.2019.11.035. Epub 2019 Dec 28. Am J Emerg Med. 2020. PMID: 31932131
Cited by
-
Understanding the circulating forms of cardiac troponin: insights for clinical practice.Clin Chem Lab Med. 2025 May 28;63(9):1667-1681. doi: 10.1515/cclm-2024-1236. Print 2025 Aug 26. Clin Chem Lab Med. 2025. PMID: 40440078 Review.
-
[Effect of co-morbid chronic kidney disease on the accuracy of cardiac troponin levels for diagnosis of acute myocardial infarction].Nan Fang Yi Ke Da Xue Xue Bao. 2023 Feb 20;43(2):300-307. doi: 10.12122/j.issn.1673-4254.2023.02.20. Nan Fang Yi Ke Da Xue Xue Bao. 2023. PMID: 36946052 Free PMC article. Chinese.
-
The use of high-sensitivity cardiac troponin T and creatinine kinase-MB as a prognostic markers in patients with acute myocardial infarction and chronic kidney disease.Ren Fail. 2023 Dec;45(1):2220420. doi: 10.1080/0886022X.2023.2220420. Ren Fail. 2023. PMID: 37278148 Free PMC article.
-
Cardiac Troponin Levels in Patients with Chronic Kidney Disease: "Markers of High Risk or Just Noise''?Diagnostics (Basel). 2024 Oct 18;14(20):2316. doi: 10.3390/diagnostics14202316. Diagnostics (Basel). 2024. PMID: 39451639 Free PMC article. Review.
References
-
- Sarnak MJ, Levey AS, Schoolwerth AC, et al. Kidney disease as a risk factor for development of cardiovascular disease: a statement from the American Heart Association councils on kidney in cardiovascular disease, high blood pressure research, clinical cardiology, and epidemiology and prevention. Circulation. 2015;108:2154–2169. doi: 10.1161/01.CIR.0000095676.90936.80. - DOI - PubMed
-
- Fox CS, Muntner P, Chen AY, et al. Acute Coronary Treatment and Intervention Outcomes Network Registry. Use of evidence-based therapies in shortterm outcomes of ST-segment elevation myocardial infarction and non–STsegment elevation myocardial infarction in patients with chronic kidney disease: a report from the National Cardiovascular Data Acute Coronary Treatment and Intervention Outcomes Network registry. Circulation. 2010;121:357–365. doi: 10.1161/CIRCULATIONAHA.109.865352. - DOI - PMC - PubMed
-
- Wybraniec MT, Bożentowicz-Wikarek M, Chudek J, et al. Pre-procedural renal resistive index accurately predicts contrast-induced acute kidney injury in patients with preserved renal function submitted to coronary angiography. Int J Cardiovasc Imaging. 2017;33(5):595–604. doi: 10.1007/s10554-016-1039-1. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
