

Long-term oncological outcomes of low anterior resection for rectal cancer with and without preservation of the left colic artery: a retrospective cohort study
- PMID: 33596860
- PMCID: PMC7890901
- DOI: 10.1186/s12885-021-07848-y
Long-term oncological outcomes of low anterior resection for rectal cancer with and without preservation of the left colic artery: a retrospective cohort study
Abstract
Background: There is uncertainty in the literature about preserving the left colic artery (LCA) during low anterior resection for rectal cancer. We analyzed the effect of preserving the LCA on long-term oncological outcomes.
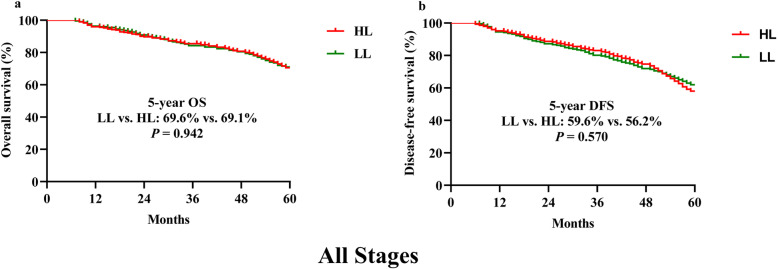
Methods: We retrospectively collected clinicopathological and follow-up details of patients who underwent low anterior resection for rectal cancer in the General Surgery Department of Guangdong Provincial People's Hospital, from January 2014 to December 2015. Cases were divided into low ligation (LL), LCA preserved, or high ligation (HL), LCA not preserved, of the inferior mesenteric artery. The 5-year overall survival (OS) and disease-free survival (DFS) rates were compared between the two groups.
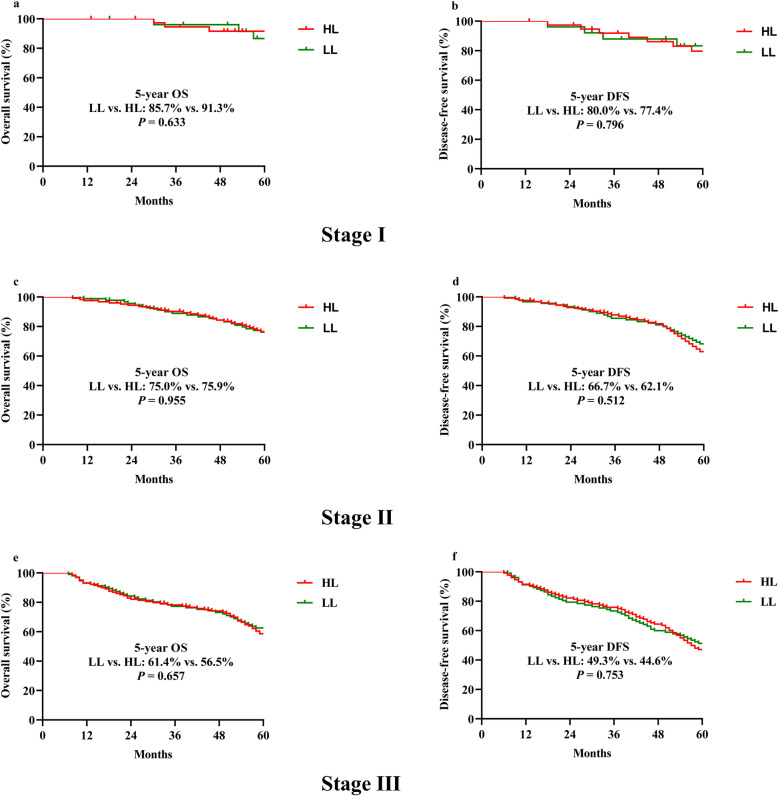
Results: Altogether, there were 221 and 295 cases in the LL group and HL groups, respectively. Operating time in the LL group was significantly longer than in the HL group (224.7 vs. 211.7 min, p = 0.039). Postoperative 30-day mortality, early complications including anastomotic leakage showed no significant differences between the LL and HL groups (postoperative 30-day mortality, 0.9% LL, 1.4% HL, p = 0.884; early complications, 41.2% LL, 38.3% HL, p = 0.509; anastomotic leakage 8.6% LL, 13.2% HL, p = 0.100). The median follow-up periods were 51.4 (7-61) months in the LL group and 51.2 (8-61) months in the HL group. During follow-up, the percentages of patients who died, had local recurrence, or had metastases were 39.8, 7.7, and 38.5%, respectively, in the LL group and 39, 8.5, and 40%, respectively, in the HL group; these differences were not significant (all p > 0.05). The 5-year OS and DFS were 69.6 and 59.6% in the LL group, respectively, and 69.1 and 56.2% in the HL group, respectively; these differences were not significant (all p > 0.05). After stratification by tumor-node-metastasis stage, the difference between the 5-year OS and DFS for stages I, II, and III cancer were not significant (all p > 0.05).
Conclusions: The long-term oncological outcomes of LL group are comparable with HL group. LL cannot be supported due to the absence of lower complication rates and the longer operating times.
Keywords: Inferior mesenteric artery; Left colic artery; Long-term oncologic outcomes; Rectal cancer.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Low Ligation of Inferior Mesenteric Artery in Laparoscopic Anterior Resection for Rectal Cancer Reduces Genitourinary Dysfunction: Results From a Randomized Controlled Trial (HIGHLOW Trial).Ann Surg. 2019 Jun;269(6):1018-1024. doi: 10.1097/SLA.0000000000002947. Ann Surg. 2019. PMID: 31082897 Clinical Trial.
-
[Effect of preservation of left colic artery on postoperative anastomotic leakage of patients with rectal cancer after neoadjuvant therapy].Zhonghua Wei Chang Wai Ke Za Zhi. 2019 Jun 25;22(6):566-572. doi: 10.3760/cma.j.issn.1671-0274.2019.06.010. Zhonghua Wei Chang Wai Ke Za Zhi. 2019. PMID: 31238636 Chinese.
-
[Long-term outcomes of laparoscopic low anterior resection of rectal carcinoma with preservation of the left colic artery].Zhonghua Wei Chang Wai Ke Za Zhi. 2017 Jun 25;20(6):660-664. Zhonghua Wei Chang Wai Ke Za Zhi. 2017. PMID: 28643311 Chinese.
-
Lymph node yield, survival benefit, and safety of high and low ligation of the inferior mesenteric artery in colorectal cancer surgery: a systematic review and meta-analysis.Int J Colorectal Dis. 2019 Jun;34(6):947-962. doi: 10.1007/s00384-019-03291-5. Epub 2019 Apr 17. Int J Colorectal Dis. 2019. PMID: 30997603
-
High ligation of the inferior mesenteric artery and anastomotic leakage in anterior resection for rectal cancer: a systematic review and meta-analysis of randomized controlled trial studies.Colorectal Dis. 2021 Mar;23(3):614-624. doi: 10.1111/codi.15419. Epub 2020 Dec 26. Colorectal Dis. 2021. PMID: 33131205
Cited by
-
Preservation versus nonpreservation of the left colic artery in anterior resection for rectal cancer: a propensity score-matched analysis.BMC Surg. 2022 May 10;22(1):164. doi: 10.1186/s12893-022-01614-y. BMC Surg. 2022. PMID: 35538516 Free PMC article.
-
Comparison of short-term surgical outcomes between high and low tie ligation of the inferior mesenteric artery in robotic rectal cancer surgery: a propensity score matching analysis.J Robot Surg. 2025 Jan 4;19(1):41. doi: 10.1007/s11701-024-02209-w. J Robot Surg. 2025. PMID: 39754668
-
Three-dimensional printing for preoperative rehearsal and intraoperative navigation during laparoscopic rectal cancer surgery with left colic artery preservation.World J Gastrointest Surg. 2024 Oct 27;16(10):3104-3113. doi: 10.4240/wjgs.v16.i10.3104. World J Gastrointest Surg. 2024. PMID: 39575297 Free PMC article.
-
Preserving the left colonic artery in radical sigmoid and rectal cancer surgery is feasible: A meta-analysis.Medicine (Baltimore). 2024 Jan 26;103(4):e37026. doi: 10.1097/MD.0000000000037026. Medicine (Baltimore). 2024. PMID: 38277569 Free PMC article.
-
Preservation of the left colic artery in modified laparoscopic anterior rectal resections without auxiliary abdominal incisions for transanal specimen retrieval.BMC Surg. 2022 Apr 21;22(1):148. doi: 10.1186/s12893-022-01593-0. BMC Surg. 2022. PMID: 35449101 Free PMC article.
References
-
- Paschke S, Jafarov S, Staib L, Kreuser ED, Maulbecker-Armstrong C, Roitman M, Holm T, Harris CC, Link KH, Kornmann M. Are colon and rectal cancer two different tumor entities? A proposal to abandon the term colorectal cancer. Int J Mol Sci. 2018;19(9):2577. doi: 10.3390/ijms19092577. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
- No. 2017A030223006, 2016A020215128/the Science and Technology Planning Project of Guangdong Province, China
- No. 201704020077/the Science and Technology Planning Project of Guangzhou, China
- NO. DFJH201913/the Second Batch of Scientific Research Projects of Dengfeng Plan
- NO. Y-2019Roche-190/the Research Fund of CSCO-Roche Oncology
- NO. Y-HS2019/2-050/the Research Fund of CSCO-Hansoh Oncology
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
