

Exit strategies: optimising feasible surveillance for detection, elimination, and ongoing prevention of COVID-19 community transmission
- PMID: 33596902
- PMCID: PMC7887417
- DOI: 10.1186/s12916-021-01934-5
Exit strategies: optimising feasible surveillance for detection, elimination, and ongoing prevention of COVID-19 community transmission
Abstract
Background: Following implementation of strong containment measures, several countries and regions have low detectable community transmission of COVID-19. We developed an efficient, rapid, and scalable surveillance strategy to detect remaining COVID-19 community cases through exhaustive identification of every active transmission chain. We identified measures to enable early detection and effective management of any reintroduction of transmission once containment measures are lifted to ensure strong containment measures do not require reinstatement.
Methods: We compared efficiency and sensitivity to detect community transmission chains through testing of the following: hospital cases; fever, cough and/or ARI testing at community/primary care; and asymptomatic testing; using surveillance evaluation methods and mathematical modelling, varying testing capacities, reproductive number (R) and weekly cumulative incidence of COVID-19 and non-COVID-19 respiratory symptoms using data from Australia. We assessed system requirements to identify all transmission chains and follow up all cases and primary contacts within each chain, per million population.
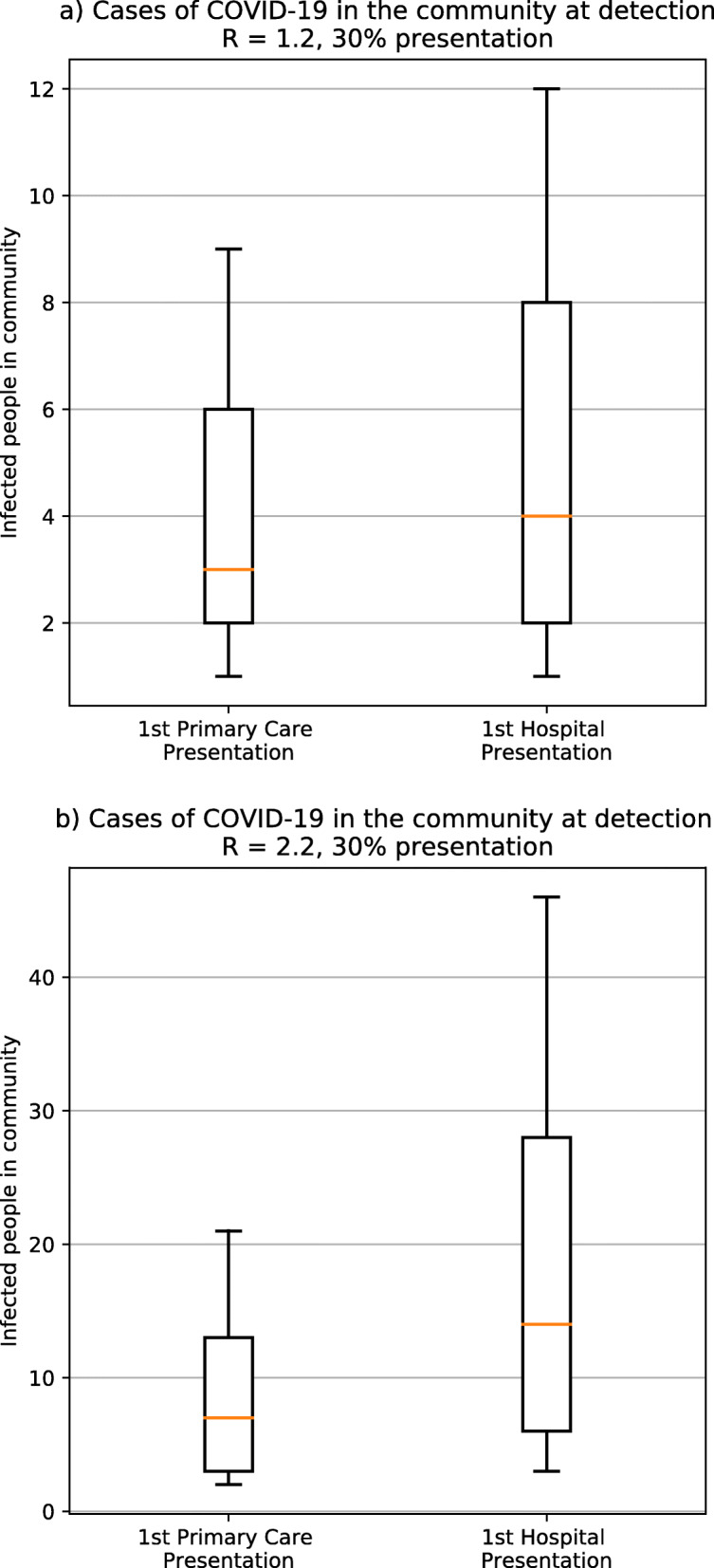
Results: Assuming 20% of cases are asymptomatic and 30% of symptomatic COVID-19 cases present for testing, with R = 2.2, a median of 14 unrecognised community cases (8 infectious) occur when a transmission chain is identified through hospital surveillance versus 7 unrecognised cases (4 infectious) through community-based surveillance. The 7 unrecognised community upstream cases are estimated to generate a further 55-77 primary contacts requiring follow-up. The unrecognised community cases rise to 10 if 50% of cases are asymptomatic. Screening asymptomatic community members cannot exhaustively identify all cases under any of the scenarios assessed. The most important determinant of testing requirements for symptomatic screening is levels of non-COVID-19 respiratory illness. If 4% of the community have respiratory symptoms, and 1% of those with symptoms have COVID-19, exhaustive symptomatic screening requires approximately 11,600 tests/million population using 1/4 pooling, with 98% of cases detected (2% missed), given 99.9% sensitivity. Even with a drop in sensitivity to 70%, pooling was more effective at detecting cases than individual testing under all scenarios examined.
Conclusions: Screening all acute respiratory disease in the community, in combination with exhaustive and meticulous case and contact identification and management, enables appropriate early detection and elimination of COVID-19 community transmission. An important component is identification, testing, and management of all contacts, including upstream contacts (i.e. potential sources of infection for identified cases, and their related transmission chains). Pooling allows increased case detection when testing capacity is limited, even given reduced test sensitivity. Critical to the effectiveness of all aspects of surveillance is appropriate community engagement, messaging to optimise testing uptake and compliance with other measures.
Keywords: COVID-19; Community transmission chains; Detection; Modelling; Primary care; Surveillance; Syndromic fever; Testing.
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- World Health Organization. Report of the WHO-China Joint Mission on Coronavirus Disease 2019 (COVID-19). 2020 16–24 February 2020.
-
- Roser M, Ritchie H, Ortiz-Ospina E. Coronavirus Disease (COVID-19) – Statistics and Research. OurWorldInDataorg. 2020. Available from: https://ourworldindata.org/coronavirus. Access date: 10 Dec 2020.
-
- covid19data.com.au. Coronavirus (COVID-19) in Australia - Cases: States and Territories 2020 [Available from: https://www.covid19data.com.au/states-and-territories. Access date: 20 Jan 2021.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
