

Tibia stress injury and the imaging appearance of stress fracture in juvenile dermatomyositis: six patients' experiences
- PMID: 33596941
- PMCID: PMC7890837
- DOI: 10.1186/s12969-021-00501-9
Tibia stress injury and the imaging appearance of stress fracture in juvenile dermatomyositis: six patients' experiences
Abstract
Background: Tibial stress injuries are frequent injuries of the lower extremity and the most common causes of exercise-induced leg pain among athletes and military recruits. They sometimes occur in patients with pathological conditions of bone metabolism such as osteoporosis or rheumatoid arthritis, but there are previously no cases reported in juvenile dermatomyositis (JDM). Here we report 6 JDM patients who presented with shin pain, and the imaging appearance of tibial stress fractures or stress reactions.
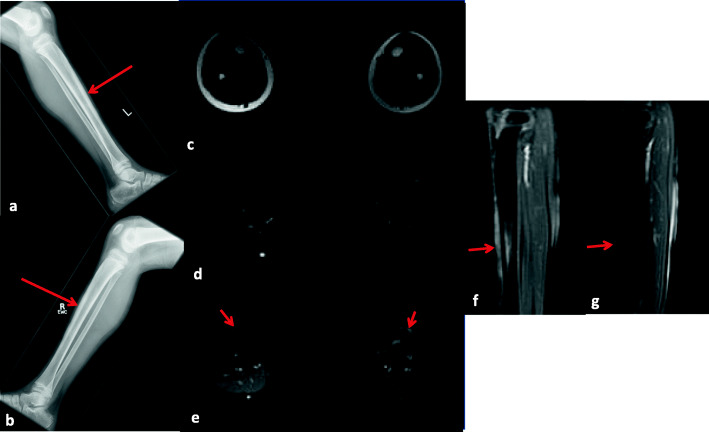
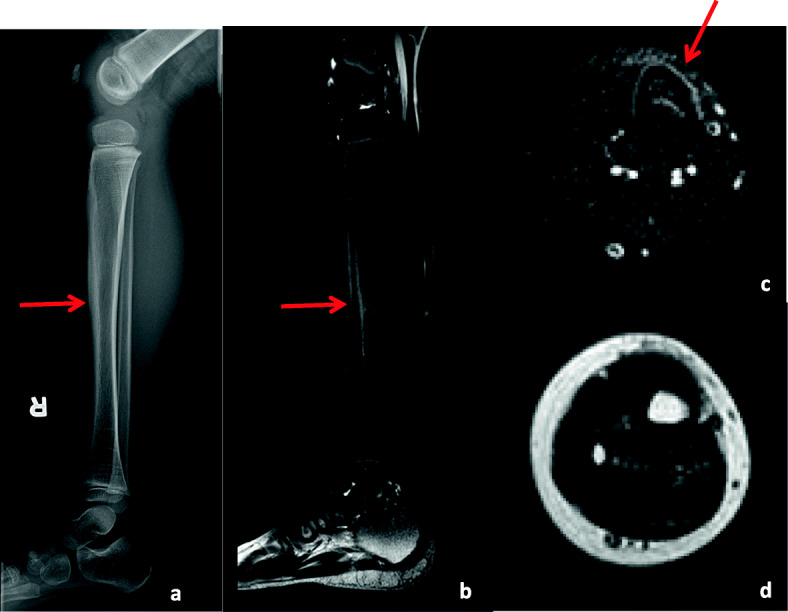
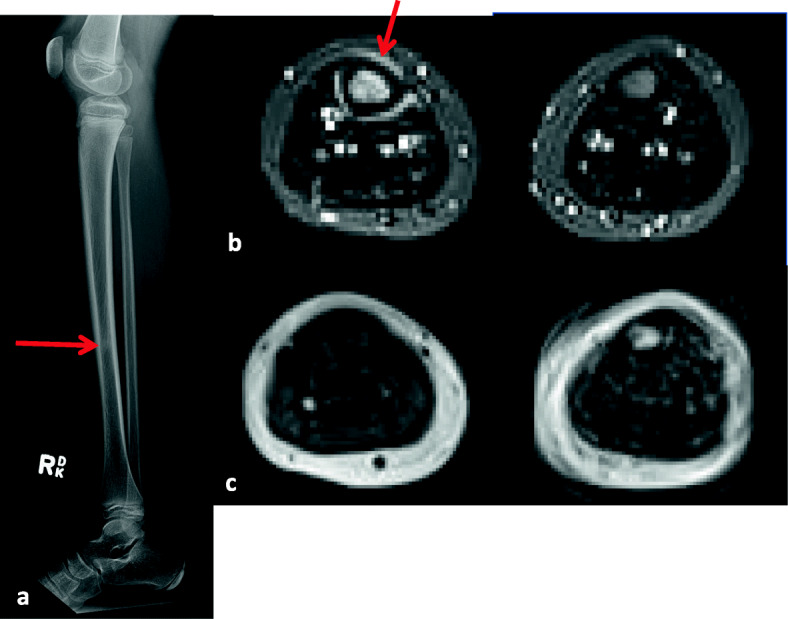
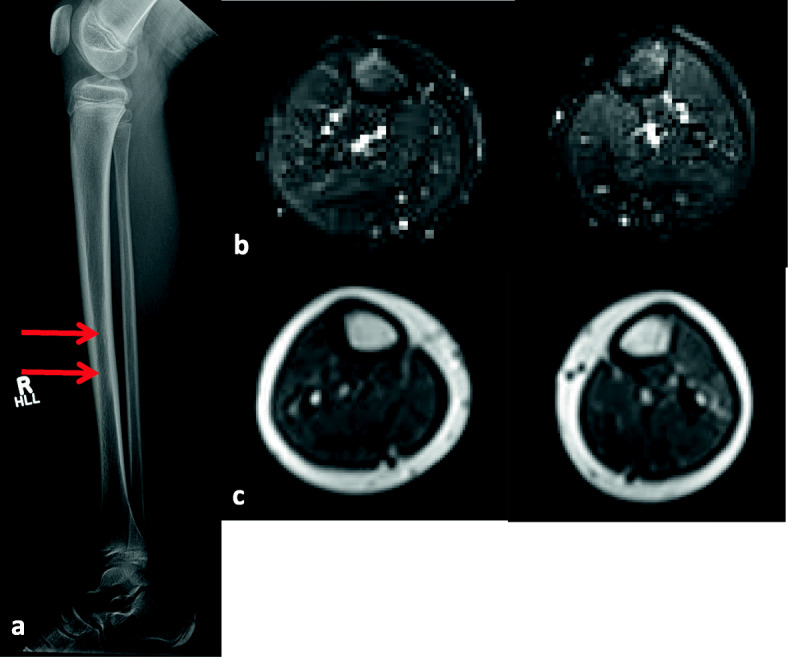
Case presentation: All 6 patients with JDM presented with shin pain or tenderness in the anterior tibia without any evidence of excessive exercise or traumatic episode. They were diagnosed with tibial stress injuries based on a combination of radiographs, three-phase bone scans, and magnetic resonance imaging (MRI), and 5 out of 6 patients had been treated with prednisone and/or methotrexate at onset of tibial stress injuries. In one patient, we could not find any abnormalities in his radiograph, but the subsequent MRI showed tibial stress reaction. In all 6 patients, the tibial stress injuries improved with only rest and/or analgesics.
Conclusion: We experienced 6 children with JDM who presented with shin pain, and who were diagnosed with tibial stress fractures or stress reactions. Their underlying disease and weakness, treatment with glucocorticoid and methotrexate, or inactivity may have resulted in these tibial injuries, and made these patients more predisposed than other children. In addition to preventing JDM patients from getting osteoporosis, we need to consider stress reactions when children with JDM complain of sudden shin pain.
Keywords: Complication; Juvenile dermatomyositis; Stress fracture; Stress reaction; Tibia; Treatment.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Keret D, Segev E, Hayek S, Lokiec F, Wientroub S. Bilateral symmetric stress fractures in a toddler. J Pediatr Orthop B. 2001;10:73–7. - PubMed
-
- Lingg GM, Soltèsz I, Kessler S, Dreher R. Insufficiency and stress fractures of the long bones occurring in patients with rheumatoid arthritis and other inflammatory diseases, with a contribution on the possibilities of computed tomography. Eur J Radiol. 1997;26:54–63. doi: 10.1016/S0720-048X(97)00039-9. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
