

Nasal nalbuphine analgesia in prehospital trauma managed by first-responder personnel on ski slopes in Switzerland: an observational cohort study
- PMID: 33596970
- PMCID: PMC7890875
- DOI: 10.1186/s13049-021-00852-y
Nasal nalbuphine analgesia in prehospital trauma managed by first-responder personnel on ski slopes in Switzerland: an observational cohort study
Abstract
Background: Pain is one of the major symptoms complained about by patients in the prehospital setting, especially in the case of trauma. When there is mountainous topography, as in Switzerland, there may be a time delay between injury and arrival of professional rescuers, in particular on ski slopes. Administration of a safe opioid by first responders may improve overall treatment. We therefore assessed administration of nasal nalbuphine as an analgesic treatment for trauma patients in Switzerland.
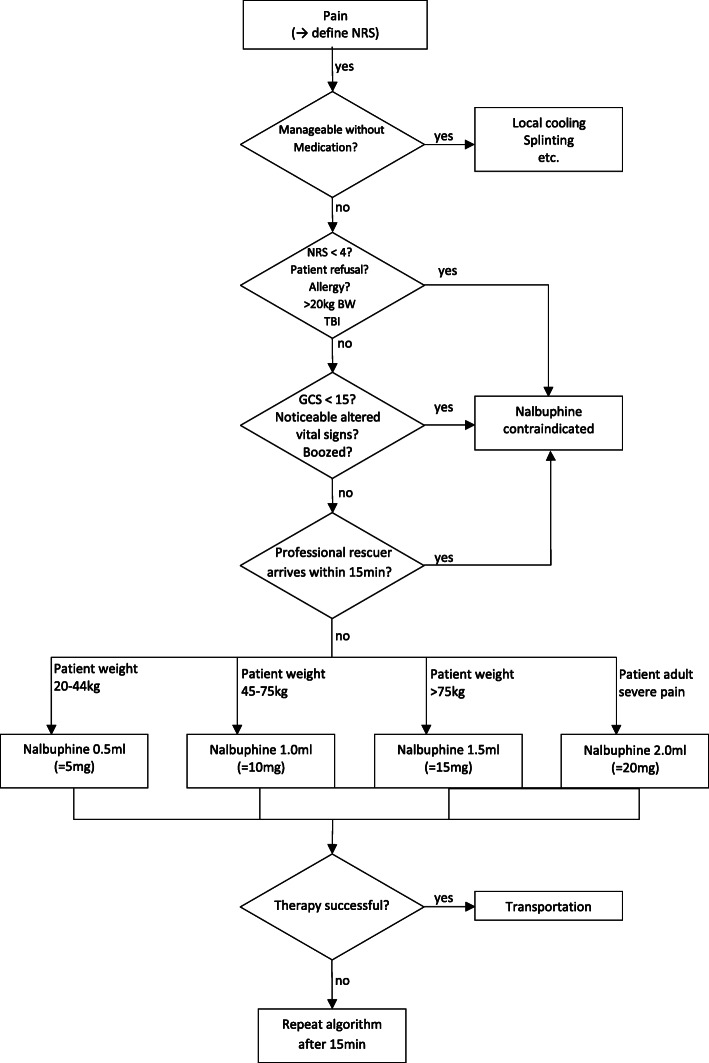
Methods: This observational cohort study examined 267 patients who were treated with nasal nalbuphine by first responders in six ski resorts in Switzerland. All first responders were instructed to begin treatment by assessing the feasibility of using nalbuphine to treat pain in the patient. A treatment algorithm was developed and distributed to assure that nalbuphine was only administered following a strict protocol. Data regarding pain scores and pain reduction after administration of nalbuphine were collected on-site. Refills were handed out to the first responders with the return of each completed questionnaire.
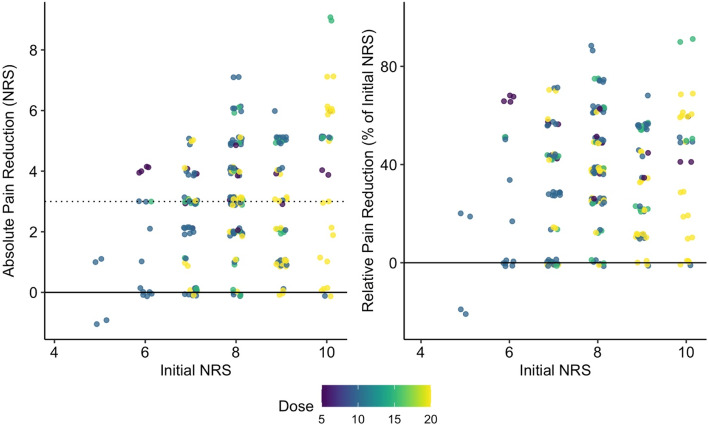
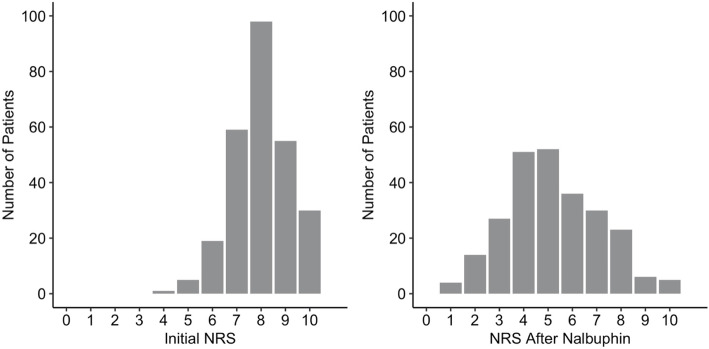
Results: Nalbuphine provided effective pain relief, with the median level of pain on the numeric rating scale for pain reduced by 3 units on average, from 8 points (p < 0.001). The multivariate regression model showed that pain reduction was more pronounced in patients with higher initial pain levels. Nalbuphine was more effective in adolsecents than in patients aged 20 to 60 years (p = 0.006). No major side effects were observed.
Conclusion: Nasal administration of nalbuphine by first responders is a presumably safe and effective noninvasive pain management strategy for acutely injured patients in the prehospital setting. This may be an alternative, especially in the case of severe pain and prolonged time between arrival of the first responders and arrival of EMS/HEMS personnel on scene.
Keywords: Emergency medicine; Nalbuphine; Pain; Prehospital analgesia; Trauma; Wilderness medicine.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Methoxyflurane in early analgesic therapy by ski patrol members on Swiss ski slopes - an observational cohort study.Scand J Trauma Resusc Emerg Med. 2024 Dec 18;32(1):132. doi: 10.1186/s13049-024-01308-9. Scand J Trauma Resusc Emerg Med. 2024. PMID: 39695854 Free PMC article.
-
Oral transmucosal fentanyl citrate analgesia in prehospital trauma care: an observational cohort study.Scand J Trauma Resusc Emerg Med. 2023 Jan 7;31(1):2. doi: 10.1186/s13049-023-01066-0. Scand J Trauma Resusc Emerg Med. 2023. PMID: 36609399 Free PMC article.
-
Effectiveness and safety of prehospital analgesia with nalbuphine and paracetamol versus morphine by paramedics - an observational study.Scand J Trauma Resusc Emerg Med. 2024 May 10;32(1):41. doi: 10.1186/s13049-024-01215-z. Scand J Trauma Resusc Emerg Med. 2024. PMID: 38730453 Free PMC article.
-
Options in prehospital analgesia.Emerg Med (Fremantle). 2002 Mar;14(1):77-84. doi: 10.1046/j.1442-2026.2002.00288.x. Emerg Med (Fremantle). 2002. PMID: 11993839 Review.
-
Prophylactic Nalbuphine to Prevent Neuraxial Opioid-Induced Pruritus: A Systematic Review and Meta-Analysis of Randomized Controlled Trials.J Perianesth Nurs. 2019 Jun;34(3):491-501.e8. doi: 10.1016/j.jopan.2018.06.098. Epub 2018 Oct 30. J Perianesth Nurs. 2019. PMID: 30389225
Cited by
-
Pharmacokinetics and tolerability of intranasal or intravenous administration of nalbuphine in infants.Arch Dis Child. 2023 Jan;108(1):56-61. doi: 10.1136/archdischild-2022-323807. Epub 2022 Sep 13. Arch Dis Child. 2023. PMID: 36100355 Free PMC article. Clinical Trial.
-
Parenteral, Non-Intravenous Analgesia in Acute Traumatic Pain-A Narrative Review Based on a Systematic Literature Search.J Clin Med. 2024 Apr 26;13(9):2560. doi: 10.3390/jcm13092560. J Clin Med. 2024. PMID: 38731088 Free PMC article. Review.
-
Methoxyflurane in early analgesic therapy by ski patrol members on Swiss ski slopes - an observational cohort study.Scand J Trauma Resusc Emerg Med. 2024 Dec 18;32(1):132. doi: 10.1186/s13049-024-01308-9. Scand J Trauma Resusc Emerg Med. 2024. PMID: 39695854 Free PMC article.
-
Oral transmucosal fentanyl citrate analgesia in prehospital trauma care: an observational cohort study.Scand J Trauma Resusc Emerg Med. 2023 Jan 7;31(1):2. doi: 10.1186/s13049-023-01066-0. Scand J Trauma Resusc Emerg Med. 2023. PMID: 36609399 Free PMC article.
-
Pilot implementation of the competence of Czech paramedics to administer sufentanil for the treatment of pain in acute trauma without consulting a physician: observational study.BMC Emerg Med. 2022 Apr 9;22(1):63. doi: 10.1186/s12873-022-00622-8. BMC Emerg Med. 2022. PMID: 35397498 Free PMC article.
References
-
- Galinski M, Ruscev M, Pommerie F, Hubert G, Srij M, Lapostolle F, Adnet F. Prise en charge de la douleur aiguë sévère chez l’adulte en médecine extrahospitalière: enquête nationale auprès des médecins de Smur. National survey of emergency management of acute pain in prehospital setting. Annales Françaises d’Anesthésie et de Réanimation. 2004;23:1149–1154. doi: 10.1016/j.annfar.2004.10.009. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
