

Surge effects and survival to hospital discharge in critical care patients with COVID-19 during the early pandemic: a cohort study
- PMID: 33596975
- PMCID: PMC7887411
- DOI: 10.1186/s13054-021-03504-w
Surge effects and survival to hospital discharge in critical care patients with COVID-19 during the early pandemic: a cohort study
Abstract
Background: The early months of the COVID-19 pandemic were fraught with much uncertainty and some resource constraint. We assessed the change in survival to hospital discharge over time for intensive care unit patients with COVID-19 during the first 3 months of the pandemic and the presence of any surge effects on patient outcomes.
Methods: Retrospective cohort study using electronic medical record data for all patients with laboratory-confirmed COVID-19 admitted to intensive care units from February 25, 2020, to May 15, 2020, at one of 26 hospitals within an integrated delivery system in the Western USA. Patient demographics, comorbidities, and severity of illness were measured along with medical therapies and hospital outcomes over time. Multivariable logistic regression models were constructed to assess temporal changes in survival to hospital discharge during the study period.
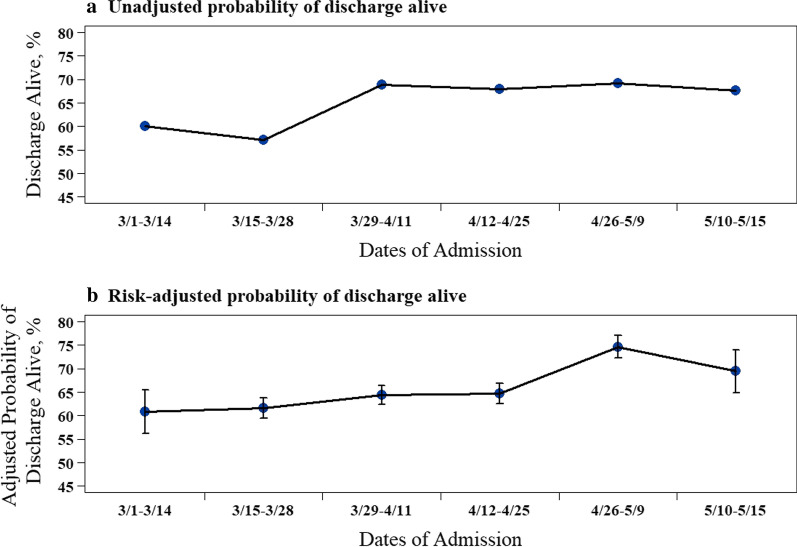
Results: Of 620 patients with COVID-19 admitted to the ICU [mean age 63.5 years (SD 15.7) and 69% male], 403 (65%) survived to hospital discharge and 217 (35%) died in the hospital. Survival to hospital discharge increased over time, from 60.0% in the first 2 weeks of the study period to 67.6% in the last 2 weeks. In a multivariable logistic regression analysis, the risk-adjusted odds of survival to hospital discharge increased over time (biweekly change, adjusted odds ratio [aOR] 1.22, 95% CI 1.04-1.40, P = 0.02). Additionally, an a priori-defined explanatory model showed that after adjusting for both hospital occupancy and percent hospital capacity by COVID-19-positive individuals and persons under investigation (PUI), the temporal trend in risk-adjusted patient survival to hospital discharge remained the same (biweekly change, aOR 1.18, 95% CI 1.00-1.38, P = 0.04). The presence of greater rates of COVID-19 positive/PUI as a percentage of hospital capacity was, however, significantly and inversely associated with survival to hospital discharge (aOR 0.95, 95% CI 0.92-0.98, P < 0.01).
Conclusions: During the early COVID-19 pandemic, risk-adjusted survival to hospital discharge increased over time for critical care patients. An association was also seen between a greater COVID-19-positive/PUI percentage of hospital capacity and a lower survival rate to hospital discharge.
Keywords: COVID-19; Critical care; Health services; Healthcare delivery; Outcomes; Surge effects.
Conflict of interest statement
No financial or non-financial competing interests exist. All study authors are employees of providence family of healthcare delivery organizations.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
